
Herausforderungen im Umgang mit unerwünschten kutanen Arzneimittelnebenwirkungen (cutaneous adverse drug reactions, CADR) – ein Fallbericht
Berliner und Münchener Tierärztliche Wochenschrift 133
DOI: 10.2376/1439-0299-2020-14
© Schlütersche Verlagsgesellschaft mbH & Co. KG. 2020
Publiziert: 08/2020
Summary
This report describes a rare case of a presumed local cutaneous drug reaction in a 10-year old, male miniature short-haired dachshund after subcutaneous injection of meloxicam and maropitant. The dog was presented with cubital joint lameness and meloxicam was injected subcutaneously. Bloody diarrhoea and bloody emesis developed over the next three days. After a repeated subcutaneous application of meloxicam and maropitant into the left thoracic wall, the skin and subcutis at the injection site indurated and became painful over an area of approx. 8x8 cm. The skin became locally necrotic and was demarcated within a few days. Histopathology of deep skin biopsies revealed severe, necrosuppurative dermatitis, panniculitis and vasculitis with marked edema and deep sequestrating pannicular necrosis. Perivascular eosinophils and vascular thrombosis were present in deeper areas of the panniculus and cutaneous muscle. Microbiological culturing failed to identify bacterial growth. Based on the treatment history, clinical changes, histopathology and the lack of laboratory data suggestive of relevant differential diagnoses, a local cutaneous adverse drug reaction (CADR) was favoured. Surgical removal of affected areas and an open wound management were successful and the dog fully recovered. This rare case of localized canine CADR illustrates the importance of a precise medical history, a strategie to exclude relevant differential diagnoses and the difficulties in ultimately confirming localized CADR in veterinary medicine.
Zusammenfassung
Der vorliegende Fall beschreibt die seltene Form einer vermuteten lokalen kutanen Arzneimittelreaktion bei einem zehnjährigen, männlichen Zwergkurzhaardackel nach subkutaner Injektion von Meloxicam und Maropitant. Der Hund erhielt aufgrund einer Ellenbogenlahmheit eine subkutane Injektion mit Meloxicam. In den darauffolgend drei Tagen entwickelte der Hund blutigen Durchfall und blutiges Erbrechen. Nach einer erneuten subkutanen Applikation von Meloxicam und Maropitant stellte sich die Haut an der Injektionsstelle der linken Brustwand nach wenigen Minuten ca. 8 x 8 cm verhärtetet und mit sehr schmerzhafter Kutis dar. Innerhalb weniger Tage wurde der veränderte Hautbereich nekrotisch und entwickelte eine Demarkation. Histopathologisch wurde eine hochgradige, ungewöhnlich tief ins Unterhautfettgewebe reichende eitrig-nekrotisierende Dermatitis, Pannikulitis und Vaskulitis mit teilweise sequestrierenden Unterhautfettgewebsnekrosen und früher, granulationsgeweblicher Demarkationstendenz sowie massiver Ödematisierung festgestellt. In tieferen Hautmuskelanteilen wurden zudem eosinophile Granulozyten und thrombosierte Blutgefäße nachgewiesen. Die mikrobiologische Untersuchung konnte kein Bakterienwachstum nachweisen. Aufgrund der Anamnese, den klinischen Veränderungen und dem Fehlen labordiagnostischer Ergebnisse, die mit einer anderen Differenzialdiagnose kompatibel gewesen wären, wurde eine lokale, kutane Arzneimittelnebenwirkung (cutaneous adverse drug reaction, CADR) vermutet. Die chirurgische Entfernung der betroffenen Areale und eine offene Wundbehandlung waren erfolgreich und es kam zur vollständigen Genesung des Hundes.
Dieser seltene Fall einer lokalen kaninen CADR stellt die Relevanz einer genauen Anamnese, eine Strategie zum Ausschluss relevanter Differenzialdiagnosen sowie die Schwierigkeiten im Nachweis einer lokalen CADR in der Tiermedizin dar.
Introduction
Adverse drug reactions (ADRs) are a feared complication in medical treatment. They are mostly subtle and characterised by short-lived symptoms, however they can also be severe and life threatening. Since 1961, the German Medical Products Act (Arzneimittelgesetz) regulates the secure distribution of pharmaceuticals for animal and humans. The law was adapted in 1976 in the aftermath of the thalidomide tragedy (Contergan® scandal), especially in respect to improving drug safety. Therefore, the drug approval procedure implicates verification of the quality, efficacy and safety of a drug. Only drugs with a positive benefit-risk-balance are approved.
Since the number of participants or animals in clinical trials is limited, very rare ADRs only first occur after approval. After approval the post marketing surveillance is in order to ensure continuous monitoring of the drug safety. Pharmaceutical companies are legally bound to inform the responsible higher federal authority, whereas veterinarians are ethically engaged when knowledge of an ADR case arises. In Germany, the Federal Office of Consumer Protection and Food Safety (BVL) is responsible for veterinary medicinal products; the Paul Ehrlich Institute (PEI) is in charge of veterinary vaccines. The reports are collected in a national database, evaluated and then forwarded to the pharmacovigilance database (EudraVigilance Veterinary) of the European Medicines Agency (EMA), where they are available for pan-European analyses. Up to 2016, 200,000 case reports for suspected drug reactions from European member states and third countries were recorded (EMA 2016); meanwhile there are more than 300,000.
ADRs can be categorised in view of different criteria. One approach distinguishes between dose-dependent and idiosyncratic reactions (Miller et al. 2013, Voie et al. 2012). Dose-dependent reactions are caused by the pharmacological properties of a drug in the sense of a specific effect associated with an active substance or excipient. The severity of the adverse effects usually correlates with the applied amount of the drug and the symptoms are deducible from the pharmacological profile of the substance (Schnyder and Pichler 2009). Idiosyncratic reactions are generally dose-independent and are presumably caused by individual immunological processes. The involvement of genetic predispositions of the affected is also presumed. Thus they are relatively uncommon, unpredictable and often linked to metabolic or enzymatic deficiencies of a patient (Miller et al. 2013). Most idiosyncratic reactions are immune-mediated and triggered by reactive metabolites and not by the drug itself (Zhang et al. 2011). The composition of these reactive metabolites can vary depending on the individual (Trepanier 2013). The manifestation of such a reaction depends on the administered drug. One hypothesis is thus not sufficient to explain all different idiosyncratic reactions. Besides epigenetic effects, the direct activation of antigen-presenting cells or the interference in the immune system’s equilibrium, oxidative stress and haptens are involved in idiosyncratic reactions (Zhang et al. 2011). A specific form of ADR is a drug eruption. Independent of a drug’s route of administration (ingestion, inhalation, injection or topical) it manifests as a cutaneous adverse drug reaction (CADR) in the skin (synonyms: cutaneous drug eruption, dermatitis medicamentosa, drug allergy) (Miller et al. 2013). With an incidence of 1–3% of hospitalised patients, the CADR is one of the most common ADRs in humans (Svensson et al. 2001). In dogs, a 2 % CADR-rate is stated regarding all canine dermatological cases in specialised dermatological clinics in the USA (Scott and Miller 1999). This presented case report describes the difficulty in diagnosing a CADR by means of an exemplary clinical course.
Case Report
Top Job:
A 10-year old, male miniature short-haired dachshund weighing 4.07 kg was presented at the Small Animal Clinic of the Freie Universität Berlin. The dog was regularly vaccinated and dewormed. Thirteen days earlier, the animal received a subcutaneous injection into the left thoracic wall of 0.2 mg/kg meloxicam (Metacam®, Boehringer Ingelheim, Germany) according to the manufacturer’s instructions. The indication was a contusion/distortion of the left cubital joint after jumping with an ensuing lameness of the left forelimb. The dog owner received Metacam®-syrup for four days of further oral treatment. The patient had a daily dose of Metacam®-syrup (1,5 mg/ml ad us. vet., oral suspension), appropriate to the body weight, administered by the syringe provided in the package. Three days after the first injection the dog showed bloody diarrhoea and the following day additional bloody emesis. The referring veterinarian again administered Metacam® in addition to maropitant (Cerenia®, Zoetis, Germany, 1mg/kg) subcutaneously, whereby both drugs were applied to the left thoracic wall. Moreover the dog received sucralfate (Sucrabest®, Combustin, Germany, 20 mg/kg BID), omeprazole (Antra Mups®, AstraZeneca, Germany, 1 mg/kg BID), clavulanate amoxicillin (Synulox®, Zoetis, Germany, 12,5 mg/kg BID), metronidazole (Metrobactin®, CP-Pharma, Germany, 25 mg/kg BID) and Pro-Kolin (Pro-Kolin+®, Albrecht, Germany, 2 ml BID) orally, for a therapy duration of seven days. The patient was infused intravenously with a balanced electrolyte solution over one day, to compensate for the loss of fluids and electrolytes and ensure the daily requirement. The gastrointestinal symptoms improved with this therapy.
A few minutes after the described renewed subcutaneous drug injection, the injection site of both drugs on the left thoracic wall showed a thickened, indurated and very painful cutis in an area of approx. 8 x 8 cm. Due to the dermal alteration, the animal was presented at the Small Animal Clinic of the Freie Universität Berlin. Goal was to find a therapy for the dermal alteration and to clarify if an ADR was aetiological.
At presentation in the clinic 13 days after the first meloxicam injection from the referring veterinarian, the dog exhibited lethargy and apathy. The vital parameters were in the norm. On the left sided transitional area between thorax and abdomen a hand-sized skin demarcation measuring approx. 8 x 8cm with multiple necrotic areas and unciform tears was observable. The area was clipped and disinfected, obvious necrotic areas were debrided under general anaesthesia by wound excision and a local wound treatment with TenderWet®24 (Paul Hartmann, Germany) was performed. The daily wound care consisted of disinfection, debridement of necrotic areas under local anaesthesia with lidocaine hydrochloride 2 % (bela-pharm, Germany) and local wound treatment with TenderWet®24. The exsiccate was forwarded to microbiological testing. The skin demarcation progressed, necessitating an excision of a ca. 6 x 6cm necrotic area under general anaesthesia on the 18th day. The resectate was histopathologically examined. Swabs were taken from the wound for microbiological testing. To prevent a spontaneous laceration of the wound, the craniodorsal, cranioventral and caudal wound margins were secured with sutures (Monocryl® 3-0 & Ethilon® 3-0, Johnson & Johnson, Germany). As desired for financial reasons by the owner, a negative-pressure wound therapy (VAC) was forgone.
The wound was locally cleansed for further 14 days, treated with Cutimed® Sorbact® (BSN medical, Germany) and subsequently closed with a suture. Twelve days later, the skin sutures were removed. The further – including long-term – healing process was complication-free.
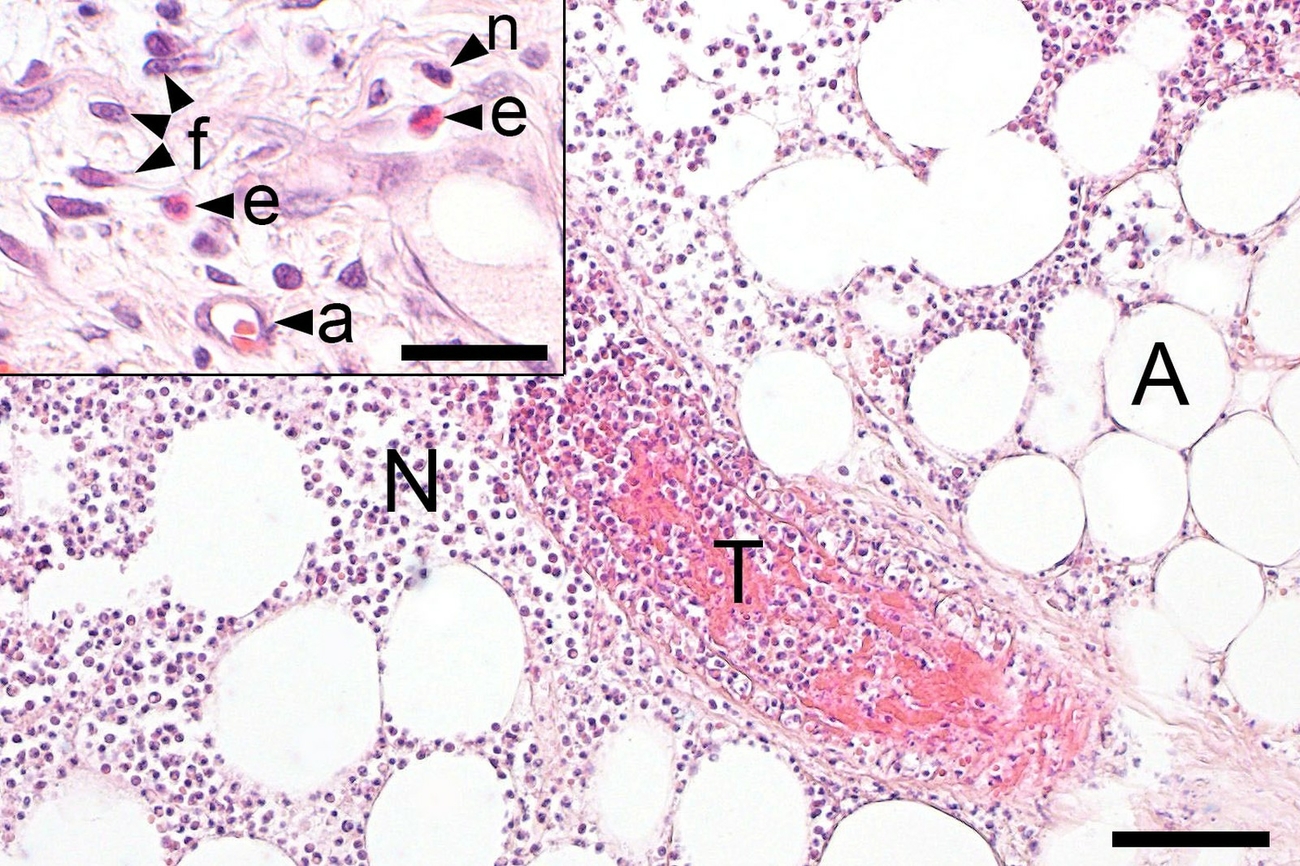
The initial blood analysis was, except for a leukocytosis with a left shift (WBC 25.02 x 109/µl, banded granulocytes absolute: 1500/µl), without appreciable changes. The microbiology of both wound secretion and resected necrotic tissue, initially and progressively excised, was negative for aerobic or anaerobic bacteria. Histology revealed marked, necrosuppurative dermatitis, panniculitis and vasculitis with an unusually deep involvement of subcutaneous adipose tissue (Fig. 1). Additionally, the process partially involved sequestrating subcutaneous adiponecrosis, a tendency to early, granulating demarcation as well as massive edema. Eosinophils and thrombosis of vessels were detected in deeper areas of skin muscle.
To classify the causality between the applied drug and the adverse reaction, the ABON-system established in veterinary medicine was used (Table 1). The necessary guidelines were developed by the Committee for Veterinary Medical Products (CVMP) of the European Medicines Agency (EMA) (see EMA/CVMP/PhVWP/552/2003 – Rev.1). In the evaluation, the chronological connection of the administration of the drug and the onset of clinical symptoms, the pharmacological / toxicological profile of the drug and possible other causes for the emergence of symptoms (other drugs, diseases) were considered. For the presented case all information are considered complete and reliable and therefore it is classified as Category B (“possible causality”).
Discussion
The presented case describes a cutaneous, presumed drug-associated complication in a male miniature smooth-haired dachshund. Possible differential diagnoses are an ADR (local reaction to meloxicam or maropitant), as well as an injection-induced abscess or phlegmon. The referring veterinarian initially suspected a CADR to the subcutaneously injected meloxicam. Meloxicam is a non-steroidal antiphlogistic drug, selectively inhibiting cyclooxygenase-2, with a long-lasting analgesic and anti-inflammatory effect (Engelhardt 1996). To date, one case of a cutaneous and ocular ADR following oral meloxicam administration in a dog has been described (Niza et al. 2007).
In the presented case, an adverse drug reaction to meloxicam cannot be ruled out. The initial symptoms began three days after the first injection of meloxicam and the subsequent oral therapy with the same drug, including bloody diarrhoea and bloody emesis. Gastrointestinal side effects are common ADRs after application of NSAIDs, which have been described in human and veterinary medicine (Gais 2018, Jones et al. 1992, Laporte et al. 2004). In very rare cases haemorrhagic diarrhoea, haematemesis and gastrointestinal ulceration have been reported as described in the summary of product characteristics of Metacam®. To what extent meloxicam affected the gastrointestinal symptoms in this case remains uncertain. A faecal parasitological examination by the referring veterinarian was positive for coccidia (Isospora canis). Coccidiosis could have been aetiological for the diarrhoea (Conboy 1998). At presentation at the clinic, the dog showed no gastrointestinal symptoms.
After a repeated subcutaneous injection of meloxicam by the referring veterinarian, cutaneous changes emerged within a few minutes. A prior sensitisation of the patient to the drug appeared to be aetiological for the rapid emergence of the dermal reaction, like described in the literature (Scott and Miller 1999).
The aetiological diagnosis of a CADR is difficult, as it can clinically resemble most dermatoses. In dogs, especially contact dermatitis, exfoliative dermatitis, pruritus, maculopapulary changes, pustules and erythema multiforme, but also severe courses with toxic epidermal necrolysis (TEN), vascular thrombosis, vasculitis as well as canine sterile neutrophilic dermatosis (Sweet’s syndrome) and canine eosinophilic dermatitis have been documented (Mason 1990; Miller et al. 2013). Thus a detailed medical history is particularly essential when dealing with acute dermatological diseases. The exact knowledge of the administered medications, the time and the route of administration are necessary to evaluate the differential diagnoses of a CADR (Miller et al. 2013). An extensive dermatological examination is necessary to describe and accurately characterise the primary skin changes. Haired skin as well as mucocutaneous junctions and the oral mucosa should be examined extensively. In the presented case, the results of the dermatological examination after the first emergence of skin changes were not documented. At presentation at the clinic, the skin changes were eight days old, necrotic with early demarcation. No inference with the initial, primary efflorescences could be drawn. An elimination of other feasible underlying dermatoses, pre-existing or intensified through the drug administration, was therefore not possible.
The symptoms of a CADR commonly manifest, as in this case, 1 - 3 weeks after initial therapy (Scott and Miller 1999). Niza et al. (2007) published a case of a canine CADR after oral meloxicam application. Here, dermal symptoms were already seen after one day (Niza et al. 2007). For other NSAIDs, cutaneous ADRs have also been described. Carprofen and firocoxib have been associated with the development of Sweet’s syndrome in four dogs (Johnson et al. 2009, Mellor et al. 2005, Vitale et al. 1999). A TEN after carprofen application in a dog has also been described (Banovic et al. 2015). Piroxicam caused epidermal ulceration in a cat (Young et al. 2018). In the presented case, it remains debatable if the NSAID meloxicam was the triggering agent for the skin changes, as maropitant was simultaneously injected subcutaneously. Maropitant is a neurokinin receptor antagonist and inhibits substance P, thus possessing a potent antiemetic effect (Benchaoui et al. 2007). According to the summary of product characteristics of the injection solution maropitant, anaphylactic reactions (allergic oedema, urticaria, erythema) may arise in rare cases. A CADR to a maropitant-injection could not be found in the literature accessible to the authors. However, it cannot be ruled out that the CADR could manifest itself easier through local tissue damage. For the orally applied antibiotic (clavulanate amoxicillin) a CADR in a dog has also been described (Porsani et al. 2017). For the other orally applied drugs, no CADRs are known to the authors.
Furthermore, a ruptured injection-induced abscess or a phlegmon must be mentioned as differential diagnoses, as a purulent-necrotic dermatitis and panniculitis was detected in histopathology of the resectate. This is very plausible in case of a secondary complication after necrosis of the skin area. A skin biopsy was not directly examined after the suspected drug reaction. This limits the validity of the histopathologic results, as the skin lesions changed macroscopically and likely also microscopically during the course of the disease. This observation underlines again the value of a histological examination of a biopsy taken at an early time after primary onset of lesions, when no interfering or distorting secondary changes are present.
Besides histopathology, performed microbiology of the wound secretion and of the resectate was negative for aerobic and anaerobic bacteria. A negative microbiological result from the wound secretion does not exclude bacterial involvement. In so-called sterile abscesses, no infectious agents are detectable. They can develop out of a foreign body reaction-induced granuloma (Cußler et al. 2014). In the presented case, the dog was treated with two antimicrobial substances for eight days before microbiological swabs were taken. A microbiological examination of the urine was not performed.
A further limiting factor was that the sample material was not shipped in a specialised transport system for the diagnosis of obligate anaerobic bacteria. It was, however, cultured for aerobic as well as obligate anaerobic bacteria. Ideally, samples should be transported and cultured with the help of specialised media when obligate anaerobes may be involved (Laboklin 2002). The antibiotics (clavulanate amoxicillin and metronidazole) given prior to the wound swab are active against aerobic and anaerobic bacteria. Hence, it is debatable to what extent bacteria may be excluded as causative agents.
The likelihood of a CADR is verified through the following factors in human medicine: the investigation of possible differential diagnoses, the temporal occurrence of clinical symptoms after drug administration, the improvement of clinical symptoms after discontinuing therapy (dechallenge), as well as the reoccurrence of symptoms after repeated drug administration (rechallenge) (Miller et al. 2013, Scott and Miller 1999). It is typical for a human CADR for skin changes to resolve within two weeks after discontinuation of therapy. In the following case, no improvement of symptoms was seen after dechallenge. A repeated administration of the previously described substances was not performed in this case. The rechallenge is regarded as the gold standard for verifying a CADR. One usually refrains from this test, due to the danger of an excessive reaction to the reapplication of the drug, as potentially fatal anaphylactic reactions are possible (Voie et al. 2012).
Besides the described ABON-System other algorithms, which employ a point system, were investigated in veterinary medicine to classify the causality between the applied drug and the adverse reaction (Hinn et al. 1998, Mauldin et al. 2006). However, the sensitivity and specificity of these algorithms have not been validated in veterinary medicine (Miller et al. 2013). The validity of these scoring systems remains controversial in human medicine. Studies on sensitivity and specificity in humans determined values of 0 % and 50 % or 53 % and 100 %, respectively (Benahmed et al. 2005a, b).
Furthermore, there are no specific changes in laboratory values, which are indicative for an ADR (Miller et al. 2013). A complete blood analysis with haemogram including differential blood count and blood chemistry should nonetheless be performed. A complete blood test can be especially helpful for diagnosing an ADR-associated haemolytic anaemia, thrombocytopenia, nephritis or hepatotoxicity as well as interpreting differential diagnoses. Eosinophilia can indicate an allergic reaction (Voie et al. 2012). In the presented case, the referring veterinarian did not perform a blood analysis. The first haemogram and differential blood count in association with this disease were performed after presentation at the clinic. There was no indication of eosinophilia.
Further laboratory analyses such as skin tests (intradermal tests, patch test, prick test), lymphocyte transformation (blastogenesis) and toxicity tests are utilised in human medicine, even if their results leave questions unanswered and their sensitivity and specificity for a diagnosis of a CADR are debatable (Miller et al. 2013, Voie et al. 2012).
Histopathologic results, likewise, serve only as an indication for a CADR, as the reaction pattern of a CADR can also arise in other aetiologies (Voie et al. 2012). The difficulty of an aetiologic diagnosis can be justified by the many different mechanisms, which can lead to a CADR. Besides direct and local toxic effects, immunopathologic hypersensitivity reactions – mostly type III or IV – can be involved, which can be associated with vasculitis, direct cytotoxic or also delayed lymphocytic reactions. In addition, mechanisms without known immunopathologies exist, like apoptosis of keratinocytes. Histology can be accordingly diverse for the pathologist. Thus, the biopsy result of the early changes can indeed be strongly indicative, yet not be evidence enough for a specific cause or mechanism. The clinical and anamnestic context is then crucial. The histology of the biopsy is nevertheless essential in every case to exclude differential aetiologies, which would require entirely different clinical management. In the here described case, a CADR in the patient is a possible cause of the observed symptoms.
Especially remarkable is the local circumscription of the described skin changes. The majority of CADRs proceed systemically with diseases such as exfoliative dermatitis, autoimmune diseases (pemphigus complex, lupus erythematodes), erythema multiforme or toxic epidermal necrolysis (Scott and Miller 1999). The local forms are more infrequent and not well described. This applies to both aetiopathogenesis and therapy. Thus, this case exemplifies the diagnostics, necessary surgical intervention and therapy of a circumscribed form of a CADR.
Due to its practical diagnostic limitations and delays, this presented case is well suited to illustrate the difficulty in verifying a cutaneous drug reaction in veterinary medicine. The therapy ultimately decided upon was successful without being able to ascertain the exact pathogenesis. Such cases should also be reported to the responsible agency to optimise the secure use of veterinary drugs and comply with due diligence set forth in the code of medical ethics outlining the notification obligation.
Acknowledgement
The authors thank Alexander Haake for his translation of the original manuscript.
Conflict of interest
There are no protected, financial, professional or other personal interests in a product, service and/or company that could influence the content or opinions expressed in the above manuscript.
Ethical approval
The dog descriped in the case report was presented at Small Animal Clinic at the Freie Universität Berlin. The owners signed a consent form to permit the diagnostic procedure, treatment of the dog and to use the collected clinical data.
Funding
We acknowledge support by the Open Access Publication Fund of the Freie Universität Berlin.
Authors contribution
CR contributed to writing the manuscript and review, undertook, additionally the postoperatively treatment. PS was the primary surgeon. MC undertook the pre- and postoperatively treatment. LB was the surgeon of the second surgery and contributed to writing and reviewing this article and did the postoperative examinations. SES and MB contributed to writing and reviewing this manuscript. ADG and JH performed the pathohistological examination and contributed to writing and reviewing this manuscript. ALB contributed to reviewing this article and performed the microbiological examinations.
Address for correspondence
Charlotte Reimann
Fachbereich Veterinärmedizin
Freie Universität Berlin
Klinik für kleine Haustiere
Oertzenweg 19B
14163 Berlin
Charlotte.Reimann@fu-berlin.de
References
Banovic F, Olivry T, Bazzle L Tobias JR, Atlee B, Zabel S, Hensel N, Linder KE (2015): Clinical and microscopic characteristics of canine toxic epidermal necrolysis. Vet Pathol 52(2): 321–330.
Benahmed S, Picot MC, Dumas F, Demoly P (2005a): Accuracy of a pharmacovigilance algorithm in diagnosing drug hypersensitivity reactions. Arch Intern Med 165(13): 1500–1505.
Benahmed S, Picot MC, Hillaire-Buys D, Blayac JP, Dujols P, Demoly P (2005b): Comparison of pharmacovigilance algorithms in drug hypersensitivity reactions. Eur J Clin Pharmacol 61(7): 537–541.
Benchaoui HA, Cox SR, Schneider RP, Boucher JF, Clemence RG (2007): The pharmacokinetics of maropitant, a novel neurokinin type-1 receptor antagonist, in dogs. J Vet Pharmacol Ther 30(4): 336–344.#
Conboy G (1998): Canine coccidiosis. Can Vet J 39(7): 443–444.
Cußler K, Bernau M, Hoffmann A (2014): Nebenwirkung an der Injektionsstelle nach Impfstoffgabe. DTBI, 1708–1712.
Engelhardt G (1996): Pharmacology of meloxicam, a new non-steroidal anti-inflammatory drug with an improved safety profile through preferential inhibition of COX-2. Br J Rheumatol 35 Suppl 1: 4–12.
Gais KS (2018): Anaphlogistika/Analgetika in der Orthopädie beim Hund. In: Klinik für kleine Haustiere des Fachbereichs Veterinärmedizin. Freie Universität Berlin, veterinärmedizinische Fakultät, Dissertation.
Hinn A, Olivry T, Luther PB, Cannon AG, Yager JA (1998): Erythema multiforme, Stevens–Johnson syndrome and toxic epidermal necrolysis in the dog: clinical classification, drug exposure, and histopathologic correlations. J Vet Allergy Clin Immunol 6: 13–20.
Johnson CS, May ER, Myers RK, Hostetter JM (2009): Extracutaneous neutrophilic inflammation in a dog with lesions resembling Sweet‘s Syndrome. Vet Dermatol 20(3): 200–205.
Jones RD, Baynes RE, Nimitz CT (1992): Nonsteroidal anti-inflammatory drug toxicosis in dogs and cats: 240 cases (1989–1990). J Am Vet Med Assoc 201(3): 475–477.
Laboklin (2002): Anaerobier: die vergessenen Bakterien? Labor für klinische Diagnostik GmbH & Co. KG, Laboklin aktuell, Info 2: 1–4.
Laporte JR, Ibanez L, Vidal X, Vendrell L, Leone R (2004): Upper gastrointestinal bleeding associated with the use of NSAIDs: newer versus older agents. Drug Saf 27(6): 411–420.
Mason KV (1990): Cutaneous drug eruptions. Vet Clin North Am Small Anim Pract 20(6): 1633–1653.
Mauldin EA, Palmeiro BS, Goldschmidt MH, Morris DO (2006): Comparison of clinical history and dermatologic findings in 29 dogs with severe eosinophilic dermatitis: a retrospective analysis. Vet Dermatol 17(5): 338–347.
Mellor PJ, Roulois AJ, Day MJ, Blacklaws BA, Knivett SJ, Herrtage ME (2005): Neutrophilic dermatitis and immune-mediated haematological disorders in a dog: suspected adverse reaction to carprofen. J Small Anim Pract 46(5): 237–242.
Miller WH, Griffin Craig E, Campbell Karen L (2013): Muller and Kirk´s Small Animal Dermatology, WB Saunders, Philadelphia, 466–472, 9.
Niza MM, Felix N, Vilela CL, Peleteiro MC, Ferreira AJA (2007): Cutaneous and ocular adverse reactions in a dog following meloxicam administration. Vet Dermatol 18(1): 45–49.
Porsani MYH, Paludetti M, Pereira CS, Haroutune Hassesian Galati L, Brunetto MA (2017): Drug reaction caused by clavulanate amoxicillin in dogs: report of two cases. MOJ Toxicol 3(5): 119–121.
Schnyder B, Pichler WJ (2009): Mechanisms of drug-induced allergy. Mayo Clin Proc 84(3): 268–272
Scott D, Miller WHJ (1999): Idiosyncratic cutaneous adverse drug reactions in the dog: Literature review and report of 101 cases (1990–1996). Canine Pract 24(5): 16–22.
Svensson C, Cowen EW, Gaspari AA (2001): Cutaneous drug reactions. Pharmacol Rev 53(3): 357–379.
Trepanier LA (2013): Idiosyncratic Drug Toxicity Affecting the Liver, Skin, and Bone Marrow in Dogs and Cats. Vet Clin North Am Small Anim Pract 43(5): 1055–1066.
Vitale C, Zenger E, Hill J (1999): Putative Rimadyl-induced neutrophilic dermatosis resembling Sweet’s syndrome in 2 dogs. Proceedings of the AAVD/ACVD Meeting Vet Dermatol; April 22–27, Maui, USA, 69–70.
Voie KL, Campbell KL, Lavergne SN (2012): Drug hypersensitivity reactions targeting the skin in dogs and cats. J Vet Intern Med 26(4): 863–874.
Young AJ, Torres SM, Koch SN (2018): Probable cutaneous adverse drug reaction to piroxicam in a cat. JFMS Open Rep 4(2): 2055116918786598.
Zhang X, Liu F, Chen X, Zhu X, Uetrecht J (2011): Involvement of the immune system in idiosyncratic drug reactions. Drug Metab Pharmacokinet 26(1): 47–59.

Kostenfreier Download
Klicken Sie hier, wenn Sie das PDF BMTW-10.23761439-0299-2020-14-Reimann.pdf (0.18 MB) herunterladen möchten
Kostenfreier Download
Klicken Sie hier, wenn Sie das PDF BMTW-10.23761439-0299-2020-14-Reimann-Tabelle1.pdf (0.12 MB) herunterladen möchten
{kind=link}