
Epidemiologie von Echinococcus multilocularis-Infektionen: Eine Übersicht zum derzeitigen Kenntnisstand und zur Situation in Deutschland
Berliner und Münchener Tierärztliche Wochenschrift 133
DOI: 10.2376/0005-9366-2020-5
© Schlütersche Verlagsgesellschaft mbH & Co. KG. 2020
Publiziert: 03/2020
Summary
Human alveolar echinococcosis (AE) and infections of foxes, raccoon dogs and dogs as the most important definitive hosts of Echinococcus (E.) multilocularis in Central Europe remain topics of general interest. Nonetheless, the incidence in humans in Germany is low (appr. 30 reported new cases per year, maximum 56 cases in 2018). Usually, the infection does not cause any clinical signs in definitive host, whereas it is often lethal in intermediate hosts, particularly in primates. Infections with E. multilocularis occur in all parts of Germany, in particular in the red fox (Vulpes vulpes); a total of 5602 cases were officially reported in Germany between 2004 and 2019. The epidemiological situation in the definitive hosts can be characterised as endemic and stable. We here review the present knowledge on the life cycle and biology of E. multilocularis and the epidemiological situation in Germany.
Zusammenfassung
Die alveoläre Echinokokkose (AE) des Menschen und Infektionen bei Fuchs, Marderhund und Hund als den in Mitteleuropa wichtigsten Endwirten von Echinococcus (E.) multilocularis, des „Kleinen Fuchsbandwurms“, stoßen in Fachkreisen, aber auch in der Öffentlichkeit immer wieder auf allgemeines Interesse. In Deutschland kommt diese Parasitose insbesondere beim Fuchs nahezu flächendeckend vor. In der Zeit von 2004 bis 2019 wurden in Deutschland 5602 Fälle gemeldet. Es ist von einer stabil-endemischen Situation auszugehen. Dennoch ist die Zahl der Neuerkrankungen von Menschen an AE gering (ca. 30 gemeldete Neuerkrankungen pro Jahr in Deutschland; Maximum: 56 berichtete Neuerkrankungen im Jahr 2018). In diesem Artikel werden der aktuelle Kenntnisstand zur Biologie und zum Lebenszyklus von E. multilocularis sowie die epidemiologische Situation in Deutschland zusammengefasst und erörtert.
Introduction
The fox tape worm Echinococcus (E.) multilocularis is considered as the cause of one of the most important parasitic zoonoses in Europe (Eckert et al. 2000,
Vuitton et al. 2015, Wen et al. 2019). Human infections can result in severe disease, characterised as alveolar echinococcosis (AE), which is usually lethal if left untreated (Vuitton et al. 2015). The incubation period of human AE has not been exactly determined, but it is assumed that it may last for periods of up to 15 years.
Many AE are only diagnosed when the disease has progressed and resulted in clinical symptoms (Gottstein et al. 2015b). Late detection of AE may affect
treatment options (Gottstein et al. 2015b, McManus et al. 2012).
Biology and life cycle
The genus Echinococcus belongs to the family Taeniidae, order Cyclophylida, in the class of Cestoda (tapeworms). In addition to E. multilocularis, the following eight species belong to the genus Echinococcus: E. granulosus sensu stricto complex (G1–G3), E. equinus (G4), E. ortleppi (G5), the clade of E. canadensis (G6–G10), E. shiquicus, E. felidis, E. oligarthra and E. vogeli. The taxonomy of the genus Echinococcus has been under continued discussion for a long time. It must therefore still be regarded as preliminary (Kinkar et al. 2017, 2018, Romig et al. 2015).
Top Job:
In Central Europe, the sylvatic life cycle of E. multilocularis dominates the epidemiological situation. It is primarily sustained by the red fox (Vulpes vulpes) and possibly by the raccoon dog (Nyctereutes procyonoides), at least in those regions, where this carnivore regularly occurs, as the main definitive hosts of the parasite (Conraths and Deplazes 2015). A number of rodents, in particular voles (Arvicolidae), serve as the main intermediate hosts (Woolsey et al. 2015a, 2015b, 2016), so that the life cycle of the parasite is coupled to a predator-prey relationship. Infections in muskrats (Ondatra zibethicus) have frequently been observed, but the potential epidemiological role of the muskrat as an intermediate host of E. multilocularis is controversially discussed (Borgsteede et al. 2003, Mathy et al. 2009, Miterpáková et al. 2006).
The domestic life cycle of E. multilocularis plays a minor, if any, role in Germany as the endemic status in the country is mainly carried by the sylvatic cycle. There is no doubt, however, that dogs (Canis lupus familiaris) are epidemiologically relevant, also for the transmission of the parasite to humans, if they serve as definitive hosts for the parasite (Kapel et al. 2006, Kern et al. 2003). The precise role of the dog in the transmission of E. multilocularis to humans is currently under discussion. It seems possible that the number of human AE cases caused by dogs is higher than often believed (Deplazes et al. 2011, Gottstein et al. 2001). In principle, cats can be definitive hosts for E. multilocularis (Knapp et al. 2016, Thompson et al. 2003), but from an epidemiological point of view, they play a minor role, if any, as the development of the parasite is retarded, worm burdens are usually low and the number of shed worm eggs is small (Kapel et al. 2006).
Humans, but also pigs (both domestic swine and wild boar) and horses represent dead-end intermediate hosts of E. multilocularis, i.e. the parasite forms ‘sterile’ metacestodes in them, which do not contain protoscolices (Bottcher et al. 2013, Peregrine, 2015). Infections with metacestodes, also under manifestation of an AE, have been reported from a large variety of further animal species, including monkeys and kangaroos, also in Germany (Brack et al. 1997, Peters et al. 2010, Rehmann et al. 2005).
Metacestodes are also regularly found in dogs, i.e. the dog can serve as a definitive or intermediate host (usually dead-end intermediate host) for E. multilocularis (Deplazes and Eckert 2001, Frey et al. 2017, Meyer et al. 2013, Peregrine 2015, Peregrine et al. 2012, Weiss et al. 2010). If a dog is only infected as an intermediate host, i.e. harbours exclusively the metacestode stage, but no adult worms in the intestine, the risk of transmission of the parasite to humans is negligible as the stage infectious for humans are the worm eggs.
The adult stages of E. multilocularis reside in the small intestine of the definitive host. They are 2–4 mm long and usually consist of five proglottids. The last, i.e. the so-called ‚gravid‘ proglottid may contain up to 300 worm eggs, which are shed into the environment with the faeces of the definitive host. If an intermediate hosts ingests infectious worm eggs, the oncospheres penetrate at the tips of the villi in the jejunum. The penetration to the Lamina propria lasts between 3 and 120 min (Thompson 2017). From the small intestine, the oncospheres reach the liver via the bloodstream primarily, less often the lungs or other organs. (Thompson 2017). During a period of one day to two weeks, the oncospheres develop there into small vesicles or cell arrays, which grow ‘infiltratively’ into the surrounding tissue. This larval stage of cestodes is called the metacestode. In the case of E. multilocularis, its growth is not limited by the Tunica adventitia of the host. As this stage consists of a large number of small vesicles and may thus resemble lung alveoli, it has historically been termed as multivesicular or alveolar. The vesicles are embedded into a dense stroma. The larval masses in the vesicles have a high viscosity.
If foxes or other potential definitive hosts eat infected rodents, the metacestodes develop into the adult stage in the small intestine of the definitive host. The last, i.e. the gravid proglottid of the adult tape worm is released after four to five weeks (prepatent period; determined in dogs, but probably in the same range in foxes and raccoon dogs). It may contain hundreds of worm eggs, which are shed with the faeces of the definitive host into the environment (Thompson 2017). It is not known, how often an adult E. multilocularis worm can release a gravid proglottid in its lifetime. Moreover, the life span of the adult worm in the intestine of the definitive host is not exactly known. It has been reported, however, that adult worms may age over a period of six to 20 months, but that they can survive for more than two years in the definitive host (Thompson 2017).
Tenacity of E. multilocularis eggs
The fact that E. multilocularis eggs can remain infectious for up to 240 days under favourable environmental conditions (mean temperature 6 °C; minimum/maximum span: -15/+27 °C) is of major epidemiological relevance (Veit et al. 1995) as the resilience of this stage supports transmission even under harsh conditions. Only at -70 °C the eggs are inactivated within 96 h and at -80 to -83 °C within 48 h (Eckert and Deplazes 2004, Veit et al. 1995). It is therefore recommended to store faecal samples, which may harbour Echinococcus eggs, or carcasses of definitive hosts that may be contaminated with them for at least four days at -70 °C or at least two days at -80 °C core temperature (Veit et al. 1995). Similar values may be valid for potentially contaminated items that cannot be decontaminated by any other means (e.g. flame treatment).
High temperatures (2 h at 55 °C or 1 h at 65 °C; 70% relative humidity) inactivate Echinococcus eggs (Federer et al. 2015). The relative humidity seems to be essential for the survival of the eggs (Laws 1968, Veit et al. 1995). Federer et al. (2015) showed that Echinococcus eggs suspended in water were only inactivated after 2 h at 65 °C, while 2 h at 43 °C were sufficient for inactivating them at a relative humidity of 15% (Veit et al. 1995). Laws (1968) investigated the resilience of Taenia pisiformis eggs to low humidity and drying out. All eggs were inactivated after incubation for 24 h at a relative humidity of 0% and a temperature of 20 °C. The same can be assumed for Echinococcus eggs.
The efficacy of common chemical disinfectants against eggs of Echinococcus spp. is controversially discussed and must therefore be regarded as uncertain
(Eckert et al. 2001). As a consequence, physical methods (dry heat, flame treatment, freezing at -80 °C for at least two days etc.) are recommended for decontamination.
Epidemiology
Europe
Echinococcus multilocularis is present in the northern hemisphere, where infections occur in Europe, Asia and parts of North America. Studies conducted in Central Europe suggest that the area, where E. multilocularis occurs, is larger than assumed until a couple of years ago. In the late 1980ies only Austria, France, Germany and Switzerland were mentioned as affected countries. Around the year 2000 it was clear that the parasite was present in at least 11 countries; in addition to the four already mentioned states, Belgium, the Czech Republic, Liechtenstein, Luxembourg, Poland, the Slovak Republic and the Netherlands were also affected (Eckert et al. 2000). In the following years, the parasite has also been detected in Denmark, Estonia and Sweden (Conraths and Deplazes 2015, Davidson et al. 2012). Oksanen and colleagues (2016) conducted a systematic review and found that E. multilocularis had by then been detected in more than 20 countries in Europe. The prevalence was high (>10%) in foxes in Estonia, France, Germany, Latvia, Liechtenstein, Lithuania, Poland, Switzerland, the Slovak Republic and the Czech Republic, while the prevalence was assessed as moderate (>1% – 10%) in Belgium, a small area in North-eastern Italy, Croatia, the Netherlands, Austria, Romania, Hungary and Ukraine. The prevalence was low (1%) in Denmark, Slovenia and Sweden. Oksanen et al. (2016) list Norway as an affected country; it should be noted, however, that the parasite has so far only been detected on Svalbard (Henttonen et al. 2001). In the EU, only the United Kingdom, Finland, Ireland and Malta were regarded as officially free from E. multilocularis (Oksanen et al. 2016).
Due to data gaps in time and space for many regions or even entire countries, it is difficult to assess if there has been a true spread of E. multilocularis in Europe. Moreover, the diagnostic techniques have changed over time and at least some of them are not sufficiently harmonised or standardised (Conraths and Deplazes 2015, Sonnenburg et al. 2017). In addition, there may be small foci, which are difficult to detect, in particular, if the prevalence is low (Staubach et al. 2011, Tackmann et al. 1998, Wahlström et al. 2015).
Germany
Until the late 1980s, only the South-western part of Germany, i.e. Baden-Wuerttemberg and the region of Swabia (Regierungsbezirk Schwaben) in Bavaria was regarded as endemic for E. multilocularis (Eckert et al. 2000). However, investigations that took place in Rhineland-Palatinate in 1982 and 1983 demonstrated the presence of E. multilocularis-infected foxes in this area, particularly in the Eifel region (Jonas and Hahn 1984). The parasite was also present in foxes in Hesse, North Rhine-Westphalia and Lower Saxony since the 1980s at the latest (Zeyhle et al. 1990). Until 1999, E. multilocularis had been detected in all German federal states except for the cities with federal state status, i.e. Berlin, Bremen and Hamburg. At this time, the eastern part of Brandenburg seemed to be almost free from E. multilocularis. Although the parasite was also detected in this region in the following years, the prevalence was lower as compared to the Northwest of this federal state. In Saxony, E. multilocularis was not detected until 1995 (Tackmann and Janitschke 1996), but the parasite was found there in the following years. Today, E. multilocularis seems to be present in the entire federal state of Saxony.
For some federal states such as Thuringia (Staubach et al. 2011), Saxony-Anhalt (Denzin et al. 2014) and Brandenburg, a spatial or temporal spread of E. multilocularis in the fox population has been demonstrated. Data of 4376 randomly sampled foxes from North-western Brandenburg, obtained from 1992 until 1995, showed two high-endemic foci with an estimated prevalence of 23.8%, while the prevalence in the surrounding area was only 4.9%. Spatial analysis of one of the foci showed that the relative risk of infection dropped drastically at a distance of 26 km from the centre of the focus, while in a radius of 5 km the risk remained high (Tackmann et al. 1998). This illustrates that small endemic foci of E. multilocularis can exist, which may be overlooked depending on the numbers of samples and the spatial distribution of the sampled animals. Parasitological post-mortem examinations of more than 700 dogs and cats from North-western Brandenburg tested all negative for E. multilocularis (K. Tackmann et al. unpublished). Examinations of 26,220 foxes in Thuringia did not only show an increase of the prevalence from 12% in 1990 to 42% in 2005, but also a spatial dissemination of E. multilocularis in the fox population. While the parasite occurred originally only in the Northwest of Thuringia, it spread over the entire territory of the federal state during the study period (Staubach et al. 2011). Since then, the epidemiological situation regarding E. multilocularis in foxes has stabilised in Thuringia at a high level (E. Meyer-Kayser and L. Hoffmann, unpublished).
A study conducted with 8459 foxes from 43 regions of Lower Saxony between 1991 and 2005, showed an increase of the mean prevalence from 12 to 20% and the presence of a stable endemic focus in the South of this federal state (Berke et al. 2008). In Saxony-Anhalt, the prevalence of E. multilocularis infected foxes rose from 13.6% (1998–2005) to 23.4% (2006–2010) (Denzin et al. 2014).
After all, it is difficult to assess, whether there was a spatial spread of E. multilocularis in Germany since the late 1980s or if intensified monitoring in foxes (and later also in raccoon dogs, at least in Eastern Germany) increased the chance of detecting infected animals. It seems also possible that both phenomena, spatial spread and intensified monitoring, overlapped. However, long-term studies from Brandenburg, Saxony-Anhalt and Thuringia argue in favour of a spatial and temporal spread (Denzin et al. 2014, Staubach et al. 2011).
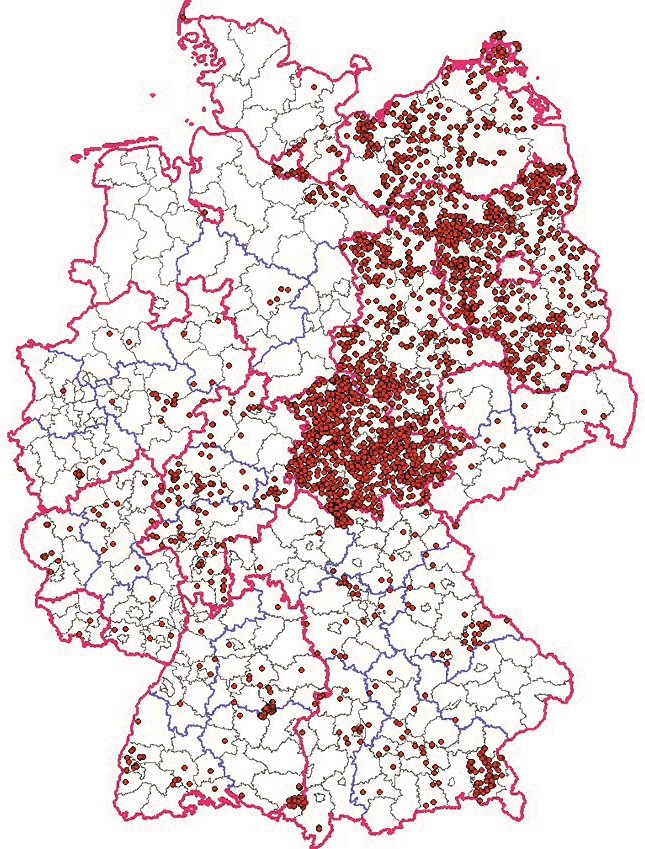
Since 1 November 2004, echinococcosis is a reportable animal disease (‘meldepflichtige Tierkrankheit’) in Germany. As of 17 January 2020, a total of 5602 cases of E. multilocularis infection were reported to the German Animal Disease Database (Tierseuchennachrichten, TSN, https://tsn.fli.de/) until 31 December 2019. During this reporting period of 15 years, the parasite was detected in all German federal states, but the number of cases varied considerably (Table 1; Fig. 1, 2). In principle, the number of reported cases does not only depend on the prevalence of the infection in the animal population, but also on the quality of the monitoring systems in individual federal states and on the motivation of the local veterinary authorities to report cases. The reported cases can therefore not be regarded as representative for the regions, from which they were reported. Moreover, monitoring activities for E. multilocularis in animals were reduced in many regions of Germany, as no significant gain of knowledge could be expected due to the stable endemic situation of E. multilocularis in foxes in the country.
Monitoring E. multilocularis infections in wildlife is a demanding task. Large sample sizes need to be obtained from the main definitive hosts (foxes and raccoon dogs), examined under high safety precautions to prevent human exposure and using laborious procedures (Conraths et al. 2003, Conraths and Deplazes 2015). It is therefore conceivable that many federal states stopped or at least reduced the intensity of the monitoring. Unfortunately, this has led to a substantial loss of knowledge regarding the epidemiological situation of E. multilocularis infections in many regions of Germany.
The distribution of E. multilocularis in various definitive hosts as reported to the German animal disease database during the period 2004–2019 is shown in Table 2. The vast majority of reported cases referred to foxes (5362; 97%). In particular in eastern parts of Germany, E. multilocularis was also regularly found in raccoon dogs (92 cases, 1.7% of all E. multilocularis-positive definitive hosts). The parasite was only rarely reported in dogs (70 cases, 1.3% of all E. multilocularis-positive definitive hosts). These findings are in accord with the results of Dyachenko et al. (2008), who studied a large non-randomised sample of dogs (n=21,588) and cats (10,650) from Germany and some other European countries and found taeniid eggs in the faeces of 0.24% of the sampled dogs (only from Germany) and 0.23% of the cats (from Germany, Denmark and the Netherlands) as well as DNA of E. multilocularis.
The number of E. multilocularis-infected intermediate hosts reported to the German animal disease database between 2004 and 2019 is relatively small (n=76; Table 3). This may be due to the facts that existing monitoring programmes focused on definitive hosts, as they shed the parasite stage that is infectious for humans, and that detection of the metacestodes is not a routine procedure when potential intermediate hosts are examined. Thus, these numbers clearly illustrate underreporting and the species distribution seems extremely biased. It must be expected that voles represent the main intermediate hosts, but these animals are only tested for E. multilocularis in dedicated research projects, not in routine monitoring. It is interesting, however, that AE was relatively frequently detected in wild boar (34 times, 44.4% of all reported cases in intermediate hosts). The fact that the infection was reported in 13 non-human primates (including three apes) illustrates the high susceptibility of these animals to infection with E. multilocularis.
Impact of E. multilocularis infection on definitive hosts
There is hardly any impact, e.g. clinical symptoms, of an E. multilocularis infection in definitive hosts, even with large worm burdens.
Diagnosis in definitive hosts
A review of the available diagnostic techniques, their performance (i.e. sensitivity and specificity) and the numbers of samples that can be processed in a specified period was published by Conraths and Deplazes (2015).
In the course of post-mortem examinations, various variants of the Intestinal Scraping Techniques (IST) are often applied, at least in Germany, in which the mucosa of the small intestine is recovered and examined for the presence of E. multilocularis specimens. To avoid exposure of the laboratory personnel to the parasite, the unopened small intestine must be frozen at -80 °C for at least two days. If the IST is used, a diagnostic sensitivity of up to 100% can be reached, if sufficient numbers of samples are taken from the small intestine of each sampled animal, preferentially from the distal part of the small intestine (Jejunum and Ileum). It should be noted, however, that the sensitivity of the IST depends heavily on the experience of the laboratory personnel and the condition of the sample (e.g. sensitivity may be reduced in autolytic samples; Tackmann et al. 2006).
For the detection of E. multilocularis in living definitive hosts, coproscopic techniques are frequently used. However, the common sedimentation/flotation technique has a low sensitivity for the detection of taeniid, including E. multilocularis, eggs (Liccioli et al. 2012). The sedimentation and sieving technique may be superior in this respect (Mathis et al. 1996). Due to the infectivity of worm eggs for humans, protective measures are mandatory, if samples from potentially infected definitive hosts are handled.
Since the eggs of E. multilocularis cannot be morphologically differentiated from other taeniid eggs, it is necessary to determine the species of taeniid eggs found in the faeces of potential definitive hosts of E. multilocularis, which can easily be done e.g. by the polymerase chain reaction (PCR) using species-specific primers (Trachsel et al. 2007; for a review, see Conraths and Deplazes, 2015). It should be noted that false-negative results are possible due to the fact that the gravid proglottid is only released in irregular intervals, i.e. intermittently, so that worm eggs are not always present in the faeces of infected definitive hosts (Kapel et al. 2006). To increase sensitivity, it may thus be useful to test also the sediment and floating material obtained by sedimentation/flotation or similar techniques by PCR to detect parasite genome in worm fragments or cells that may also be shed with the faeces.
Impact of E. multilocularis infection on intermediate hosts
Infection of intermediate hosts with E. multilocularis leads to the clinical picture of AE. Its primary manifestation is almost always in the liver, but the incubation period can vary over a wide range. It seems that it can be as high as 15 years in humans (Kern et al. 2017).
Diagnosis in intermediate hosts
In the first instance, medical imaging techniques, which allow detecting macroscopically visible alterations, particularly in the liver, can be used as a screening method. Biopsies can then be taken from such alterations and examined histologically and tested by PCR for genome fragments of E. multilocularis. Taking biopsies from suspect AE material requires special surgical precautions to prevent the spread of metacestode tissue in the body. Moreover, serological methods are available, which allow the detection of antibodies directed against E. multilocularis in intermediate hosts including aberrant intermediate hosts (Conraths and Deplazes 2015, Siles-Lucas et al. 2017). Usually, these tests are validated for use with human serum samples. If sera of other species are to be tested, the assays may have to be adapted and appropriately validated.
Treatment of dogs and cats
Any treatment of E. multilocularis-infected dogs requires strict hygienic measures to prevent infections of humans or intermediates hosts. This risk is much lower in cats. Praziquantel (e.g. 5 mg/kg body mass orally or 5.7 mg/kg intramuscularly in dogs and cats) is highly efficacious against adult E. multilocularis (Thomas and Gönnert, 1978), but epsiprantel can also be used (Eckert et al. 2001). It must be stressed, however, that these substances have no ovicidal effect, so that shed eggs remain infectious. Faeces passed after treatment must therefore by safely disposed of.
In endemic areas (i.e. most of Germany), re-infections may occur at any time. In such regions, appropriate information on the epidemiological situation should be provided to the public. Dog holders can be advised not to let their pets roam freely, so that they cannot prey on potentially infected intermediate hosts. If definitive hosts have a chance to prey on potentially infected intermediate hosts, it is advisable to treat them within the prepatent period, i.e. every four weeks.
Risk factors for the infection of foxes with E. multilocularis
When environmental factors were analysed for their potential impact on the infection of foxes with E. multilocularis, it became evident that foxes that had been shot in the vicinity of waterbodies or in areas with a high proportion of pastures were significantly more frequently infected with E. multilocularis than foxes shot under other environmental conditions (Staubach et al. 2001). However, attempts to predict risk areas for the infection of foxes on the basis of landscape data in Germany were not yet successful.
Fox populations were believed to have increased in many areas in the past. This was at least in part due to human intervention, e.g. the oral immunisation of foxes against rabies, the elimination of potentially competing predators (e.g. the lynx and until recently also the wolf), the feeding of wild animals and a limited hunting pressure, at least as far as carnivores are concerned (Hegglin et al. 2015). Foxes were also successful in colonising urban areas. There is epidemiological evidence indicating that the contamination of the environment with eggs of E. multilocularis has substantially increased in Zurich, Switzerland, due to the rising number of urban foxes (Hofer et al. 2000). However, the food resources available to foxes in an urban situation (waste and a spectrum of rodent species that is different from rural areas) may support the life cycle of the parasite in central urban areas less efficiently than in peripheral or rural regions, which may result in a lower prevalence of E. multilocularis in foxes in the city centres (Liccioli et al. 2015, Peter Deplazes, personal communication). This may also explain the fact that E. multilocularis has so far not been detected in the city centre of Berlin, while the parasite has been present in the periphery and in neighbouring counties in Brandenburg, in particular north and north-west of Berlin, for a long time (Tackmann and Janitschke 1996, Tackmann et al. 1998).
Control of E. multilocularis in foxes
In some areas, the prevalence of E. multilocularis in the fox population was substantially decreased by distributing praziquantel-containing baits, which are taken up by the foxes (Comte et al. 2013, König et al. 2019, Tackmann et al. 2001). However, this method is laborious and expensive, as repeated treatments in relatively short intervals of six weeks to three months are necessary. Moreover, there is the risk of re-invasion of the parasite from adjacent endemic regions or the re-emergence of the infection if control is not perfect or if infected intermediate hosts remain in the area. Yet, the method may substantially reduce the prevalence and thus the risk of human infection, even if eradication of E. multilocularis is not achieved (Hegglin and Deplazes 2013). By contrast, increased hunting of foxes failed to reduce the prevalence in the remaining population in France (Comte et al. 2017). On the contrary, the E. multilocularis prevalence increased in the area with increased hunting pressure, possibly by immigration of infected animals from the surroundings or due to an increasing number of rodents that represent intermediate hosts for the parasite.
Human Alveolar Echinococcosis
Several review articles have been published on clinical aspects of human AE (Brehm 2017, Gottstein et al. 2015a, Stojkovic and Junghanss 2013, Vuitton et al. 2015, Vuitton et al. 2003, Wen et al. 2019), the epidemiological situation of human AE (Baumann et al. 2019, Deplazes et al. 2017, Eckert 1996, Eckert et al. 2000, Eckert and Deplazes 2004, Eckert and Thompson 2017) and its general impact on human health (Torgerson 2003, Torgerson and Budke 2003, Torgerson et al. 2010).
The clinical picture of AE is caused by the ‘infiltrative’ growth of the metacestode stage, which normally invades the liver, into the surrounding tissue, comparable to a malign neoplasia. In addition, ‘metastatic’ metacestode growth may occur, if parasite tissue of this stage is released and transported through blood or lymph vessels to distant organs such as brain, lungs or bones.
Alveolar echinococcosis therefore represents a severe and life-threatening disease, although it is a rare condition, at least in Europe. It has been estimated that the incidence ranges between 170 and 200 new human AE cases per year, with a focus in France, Germany, Lithuania, Poland and Switzerland (Palmer 2011). In Germany, approximately 30 new AE cases per year were reported on average since 2001 (maximum: 56 cases in 2018) to the German Robert Koch-Institut (SurvStat@RKI 2.0, https://survstat.rki.de, accessed 06 February 2020). However, substantial underreporting in Germany has been suspected (Jorgensen et al. 2008).
Human AE is diagnosed by serology and a combination of medical imaging techniques with biopsies, which are then further tested for E. multilocularis by PCR or histology. Diagnosis and therapy of human AE should be conducted in specialised hospitals or clinical centres. There are international and national guidelines regarding diagnostic and therapeutic procedures for AE (Anonymus 1996, Brunetti et al. 2010, Kern et al. 2000a, 2000b, Kern 2006, 2010, Kern et al. 2000a, 2000b, Kratzer et al. 2019, Thomas et al. 2017).
Early diagnosis and therapy substantially increase the chance for treatment success, which usually consists of a combination of surgical intervention (resection of the affected parts of the liver, if possible) with long-term albendazole treatment. A relative survival analysis undertaken in Switzerland with data from 155 representative cases came to the conclusion that the life expectancy for an average 54-year-old patient diagnosed with AE in 1970 was reduced by 18.2 and 21.3 years for men and women, respectively. By 2005, the reduction in life expectancy was only 3.5 and 2.6 years, respectively. Patients who had undergone radical surgery had a better outcome and the prognosis was better in young as compared to old patients (Torgerson et al. 2008). In conclusion, AE can nowadays be successfully treated, but it is essential to diagnose and treat the disease as early as possible. It usually remains fatal, however, if left untreated.
Risk factors for human AE
A systematic review and meta-analysis of published studies showed at the global level that the following main potential risk factors were associated with human AE: dog or cat ownership, having a kitchen garden, haymaking in meadows not adjacent to water, going to forests for vocational reasons, occupation farmer and handling foxes (Conraths et al. 2017). A study conducted in Germany yielded similar results (Kern et al. 2004).
Analysis of data on human AE available in the European Registry on Echinococcosis, which was initiated in 1998, included 559 patients followed between 1982 and 2000 (Kern et al. 2003). Most patients with diagnosed AE in the database had lived in rural areas between eastern France and western Austria, but sporadic cases scattered over Europe, also outside the known endemic regions. Of 210 patients with known profession, 61.4% had been active in vocational or part-time farming, gardening, forestry or hunting. The mean age, at which the patients were diagnosed with AE, was 52.5 years; 78% of them showed symptoms. In them, AE primarily manifested as a disease of the liver. In 190 patients (34%), metacestode tissue had already spread. In 2000, when the study ended, 408 (73%) patients were still alive and 4.9% were regarded as cured.
More recently, Vuitton et al. (2015) found that the number of AE cases had risen in some areas long known as endemic for E. multilocularis (Austria, France, Germany and Switzerland) and that AE was in the meantime also found in regions, where the disease had not been found in humans before, in particular in central and eastern European countries and the Baltic states (Vuitton et al. 2015). Gottstein et al. (2015a) anticipated a future increase of AE in humans, and called for scaling-up research to improve the development and implementation of prevention measures, early diagnosis and curative treatment of human AE rapidly.
Prevention of human AE
Prevention of human AE is best achieved by reducing or avoiding the risk of exposure to E. multilocularis eggs, in particular the risk of ingesting them.
Depending on the accepted risk level, people can be advised to eat only sufficiently heated berries, windfall and vegetables, if they may be contaminated with E. multilocularis eggs, e.g. through fox faeces. If a slightly increased risk is accepted, these types of food can be thoroughly washed before they are eaten. People handling potentially infected definitive hosts, in particular foxes and raccoon dogs, should adopt protective measures such as wearing gloves. Dogs with access to potentially infected rodents can be treated with praziquantel within the prepatent period of E. multilocularis (appr. four weeks), thus avoiding patent infections of the dog. Faeces of potentially infected dogs should be removed and disposed of safely, i.e. they must not be accessible to intermediate hosts. Guidelines of the Robert Koch-Institut for physicians provide further advice (RKI Ratgeber Echinokokkose).
Acknowledgements
We would like to thank our colleagues in the veterinary investigation centres of the German federal states for investigating definitive and intermediate hosts of E. multilocularis for long periods, sometimes decades, and for reporting the results to the German Animal Disease Database (TSN). We also thank Dr. habil. Christine Klaus for initiating this article and for helpful comments and suggestions. We are indebted to Dr. Elisabeth Meyer-Kayser and Dr. Lothar Hoffmann, Thüringer Landesamt für Verbraucherschutz, who gave us access to unpublished data and to Dr. Carolina Probst for her critical review of the manuscript. We gratefully acknowledge the work of Dr. Kirsten Tackmann, who founded and primed the research regarding the epidemiology of E. multilocularis in Germany at the FLI.
Conflict of interest
The authors declare that they have no conflicts of interest. The authors declare that they have no affiliations with or involvement in any organization or entity with any financial interest in the subject matter or materials discussed in this manuscript.
Ethical approval
Since this is a literature review and analysis of officially data reported, no ethical vote was necessary. The authors declare that no research interventions or experiments with animals or human beings, no clinical trials as well as no clinical research were conducted in the context of this study.
Funding
The authors declare that they had no financial support for this publication. We agree to make all data available upon reasonable request.
Authors’ contribution
FJC: Project idea and development, literature search and review, data analysis, manuscript writing, manuscript editing. PM: Project development, literature search and review, manuscript writing, manuscript editing. All authors corrected and approved the final version.
Address for correspondence
Prof. Dr. Franz J. Conraths
Friedrich-Loeffler-Institut
Institute of Epidemiology
Südufer 10
17493 Greifswald-Insel Riems
franz.conraths@fli.de
References
Anonymus (1996): Guidelines for treatment of cystic and alveolar echinococcosis in humans. WHO Informal Working Group on Echinococcosis. Bull World Health Organ 74: 231–242.
Baumann S, Shi R, Liu W, Bao H, Schmidberger J, Kratzer W, Li W; interdisciplinary Echinococcosis Working Group Ulm (2019): Worldwide literature on epidemiology of human alveolar echinococcosis: a systematic review of research published in the twenty-first century. Infection 47: 703–727.
Berke O, Romig T, von Keyserlingk M (2008): Emergence of Echinococcus multilocularis among Red Foxes in northern Germany, 1991–2005. Vet Parasitol 155: 319–322.
Borgsteede FHM, Tibben JH, van der Giessen JWB (2003): The musk rat (Ondatra zibethicus) as intermediate host of cestodes in the Netherlands. Vet Parasitol 117: 29–36.
Bottcher D, Bangoura B, Schmaschke R, Muller K. Fischer S, Vobis V, Meiler H, Wolf G, Koller A, Kramer S, Overhoff M, Gawlowska S, Schoon HA (2013): Diagnostics and epidemiology of alveolar echinococcosis in slaughtered pigs from large-scale husbandries in Germany. Parasitol Res 112: 629–636.
Brack M, Tackmann K, Conraths FJ, Rensing S (1997): Alveolar hydatidosis (Echinococcus multilocularis) in a captive rhesus monkey (Macaca mulatta) in Germany. Trop Med Int Health 2: 754–759.
Brehm K (2017): Die Echinokokkose – Eine Übersicht und neue Erkenntnisse in der Diagnostik, Therapie und Parasitenbiologie. RKI Epid Bull 15: 127–132.
Brunetti E, Kern P, Vuitton DA; Writing Panel for the WHO-IWGE (2010): Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop 114: 1–16.
Comte S, Raton V, Raoul F, Hegglin D, Giraudoux P, Deplazes P, Favier S, Gottschek D, Umhang G, Boue F, Combes B (2013): Fox baiting against Echinococcus multilocularis. Contrasted achievements among two medium size cities. Prev Vet Med 111: 147–155.
Comte S, Umhang G, Raton V, Raoul F, Giraudoux P, Combes B, Boué F (2017): Echinococcus multilocularis management by fox culling: An inappropriate paradigm. Prev Vet Med 147: 178–185.
Conraths FJ, Staubach C, Tackmann K (2003): Statistics and sample design in epidemiological studies of Echinococcus multilocularis in fox populations. Acta Trop 85: 183–189.
Conraths FJ, Deplazes P (2015): Echinococcus multilocularis. Epidemiology, surveillance and state-of-the-art diagnostics from a veterinary public health perspective. Vet Parasitol 213: 149–161.
Conraths FJ, Probst C, Possenti A, Boufana B, Saulle R, La Torre G, Busani L, Casulli A (2017): Potential risk factors associated with human alveolar echinococcosis. Systematic review and meta-analysis. PLoS Negl Trop Dis 11, e0005801.
Davidson RK, Romig T, Jenkins E, Tryland M, Robertson LJ (2012): The impact of globalisation on the distribution of Echinococcus multilocularis. Trends Parasitol 28: 239–247.
Denzin N, Schliephake A, Frohlich A, Ziller M, Conraths FJ (2014): On the move? Echinococcus multilocularis in red foxes of Saxony-Anhalt (Germany). Transbound Emerg Dis 61: 239–246.
Dyachenko V, Pantchev N, Gawlowska S, Vrhovec MG, Bauer C (2008): Echinococcus multilocularis infections in domestic dogs and cats from Germany and other European countries. Vet Parasitol 157: 244–253.
Deplazes P, Eckert J (2001): Veterinary aspects of alveolar echinococcosis – a zoonosis of public health significance. Vet Parasitol 98: 65-87.
Deplazes P, van Knapen F, Schweiger A, Overgaauw PA (2011): Role of pet dogs and cats in the transmission of helminthic zoonoses in Europe, with a focus on echinococcosis and toxocarosis. Vet Parasitol 182: 41–53.
Deplazes P, Rinaldi L, Alvarez Rojas CA, Torgerson PR, Harandi MF, Romig T, Antolova D, Schurer JM, Lahmar S, Cringoli G, Magambo J, Thompson RC, Jenkins EJ (2017): Global Distribution of Alveolar and Cystic Echinococcosis. Adv Parasitol 95: 315–493.
Eckert J (1996): [The “dangerous fox tapeworm” (Echinococcus multilocularis) and alveolar echinococcosis of humans in central Europe]. Berl Munch Tierarztl Wochenschr 109: 202–210.
Eckert J, Conraths FJ, Tackmann K (2000): Echinococcosis: an emerging or re-emerging zoonosis? Int J Parasitol 30: 1283–1294.
Eckert J, Deplazes P (2004): Biological, epidemiological, and clinical aspects of echinococcosis, a zoonosis of increasing concern. Clin Microbiol Rev 17: 107–135.
Eckert J, Gottstein B, Heath D, Liu F-J (2001): Prevention of echinococcosis in humans and safety precautions. In: Eckert J, Gemmell MA, Meslin F-X, Pawlowsky ZS (eds.), WHO/OIE Manual on Echinococcosis in Humans and Animals: a Public Health Problem of Global Concern. World Organisation for Animal Health, Paris, 238–247.
Eckert J, Thompson RC, Bucklar H, Bilger B, Deplazes P (2001): [Efficacy evaluation of epsiprantel (Cestex) against Echinococcus mutilocularis in dogs and cats]. Berl Munch Tierarztl Wochenschr 114:121-126.
Eckert J, Thompson RC (2017): Historical Aspects of Echinococcosis. Adv Parasitol 95: 1–64.
Federer K, Armua-Fernandez MT, Hoby S, Wenker C, Deplazes P (2015): In vivo viability of Echinococcus multilocularis eggs in a rodent model after different thermo-treatments. Exp Parasitol 154: 14–19.
Frey CF, Marreros N, Renneker S, Schmidt L, Sager H, Hentrich B, Milesi S, Gottstein B (2017): Dogs as victims of their own worms: Serodiagnosis of canine alveolar echinococcosis. Parasit Vectors 10: 422.
Gottstein B, Saucy F, Deplazes P, Reichen J, Demierre G, Busato A, Zuercher C, Pugin P (2001): Is high prevalence of Echinococcus multilocularis in wild and domestic animals associated with disease incidence in humans? Emerg Infect Dis 7: 408–412.
Gottstein B, Stojkovic M, Vuitton DA, Millon L, Marcinkute A, Deplazes P (2015a): Threat of alveolar echinococcosis to public health – a challenge for Europe. Trends Parasitol 31: 407–412.
Gottstein B, Wang J, Boubaker G, Marinova I, Spiliotis M, Muller N, Hemphill A (2015b): Susceptibility versus resistance in alveolar echinococcosis (larval infection with Echinococcus multilocularis). Vet Parasitol 213: 103–109.
Hegglin D, Bontadina F, Deplazes P (2015): Human-wildlife interactions and zoonotic transmission of Echinococcus multilocularis. Trends Parasitol 31: 167–173.
Hegglin D, Deplazes P (2013): Control of Echinococcus multilocularis. Strategies, feasibility and cost-benefit analyses. Int J Parasitol 43: 327–337.
Henttonen H, Fuglei E, Gower CN, Haukisalmi V, Ims RA, Niemimaa J, Yoccoz NG (2001): Echinococcus multilocularis on Svalbard: introduction of an intermediate host has enabled the local life-cycle. Parasitology 123: 547–552.
Hofer S, Gloor S, Müller U, Mathis A, Hegglin D, Deplazes P (2000): High prevalence of Echinococcus multilocularis in urban red foxes (Vulpes vulpes) and voles (Arvicola terrestris) in the city of Zürich, Switzerland. Parasitology 120: 135–142.
Jonas D, Hahn W (1984): Nachweis von Echinococcus multilocularis in Rheinland-Pfalz. Der Prakt Tierarzt 65: 64–69.
Jorgensen P, an der Heiden M, Kern P, Schöneberg I, Krause G, Alpers K (2008): Underreporting of human alveolar echinococcosis, Germany. Emerg Infect Dis 14: 935–937.
Kapel CM, Torgerson PR, Thompson RC, Deplazes P (2006): Reproductive potential of Echinococcus multilocularis in experimentally infected foxes, dogs, raccoon dogs and cats. Int J Parasitol 36: 79–86.
Kern P (2006): Medical treatment of echinococcosis under the guidance of Good Clinical Practice (GCP/ICH). Parasitol Int 55 (Suppl): S273–282.
Kern P (2010): Clinical features and treatment of alveolar echinococcosis. Curr Opin Infect Dis 23: 505–512.
Kern P, Kratzer W, Reuter S (2000a): [Alveolar echinococcosis: diagnosis]. Dtsch Med Wochenschr 125: 59–62.
Kern P, Kratzer W, Reuter S (2000b): [Alveolar echinococcosis: therapy]. Dtsch Med Wochenschr 125: 87–89.
Kern P, Ammon A, Kron M, Sinn G, Sander S, Petersen LR, Gaus W (2004): Risk factors for alveolar echinococcosis in humans. Emerg Infect Dis 10: 2088–2093.
Kern P, Bardonnet K, Renner E, Auer H, Pawlowski Z, Ammann RW, Vuitton DA, Kern P (2003): European echinococcosis registry: human alveolar echinococcosis, Europe, 1982–2000. Emerg Infect Dis 9: 343–349.
Kern P, Menezes da Silva A, Akhan O, Müllhaupt B, Vizcaychipi KA, Budke C, Vuitton DA (2017): The Echinococcoses: Diagnosis, Clinical Management and Burden of Disease. Adv Parasitol 96: 259–369.
Kinkar L, Laurimäe T, Acosta-Jamett G, Andresiuk V, Balkaya I, Casulli A, Gasser RB, van der Giessen, J, González LM, Haag KL, Zait H, Irshadullah M, Jabbar A, Jenkins DJ, Kia EB, Manfredi MT, Mirhendi H, M’rad S, Rostami-Nejad M, Oudni-M’rad M, Pierangeli NB, Ponce-Gordo F, Rehbein S, Sharbatkhori M, Simsek S, Soriano SV, Sprong H, Šnábel V, Umhang G, Varcasia A, Saarma U (2018): Global phylogeography and genetic diversity of the zoonotic tapeworm Echinococcus granulosus sensu stricto genotype G1. Int J Parasitol 48: 729–742.
Kinkar L, Laurimäe T, Sharbatkhori M, Mirhendi H, Kia EB, Ponce-Gordo F, Andresiuk V, Simsek S, Lavikainen A, Irshadullah M, Umhang G, Oudni-M‘rad M, Acosta-Jamett G, Rehbein S, Saarma U (2017): New mitogenome and nuclear evidence on the phylogeny and taxonomy of the highly zoonotic tapeworm Echinococcus granulosus sensu stricto. Infect Genet Evol 52: 52–58.
Knapp J, Combes B, Umhang G, Aknouche S, Millon L (2016): Could the domestic cat play a significant role in the transmission of Echinococcus multilocularis? A study based on qPCR analysis of cat feces in a rural area in France. Parasite 23: 42
König A, Romig T, Holzhofer E (2019): Effective long-term control of Echinococcus multilocularis in a mixed rural-urban area in southern Germany. PloS One 14: e0214993.
Kratzer W, Schmidberger J, Hillenbrand A, Henne-Bruns D, Gräter T, Barth TFE, Grüner B (2019): Alveoläre Echinokokkose: Eine Herausforderung für Diagnostik, Therapie und Klinisches Management. RKI Epid Bull 41: 423–430.
Laws GF (1968): Physical factors influencing survival of taeniid eggs. Exp Parasitol 22: 227–239.
Liccioli S, Catalano S, Kutz SJ, Lejeune M, Verocai GG, Duignan PJ, Fuentealba C, Ruckstuhl KE, Massolo A (2012): Sensitivity of double centrifugation sugar fecal flotation for detecting intestinal helminths in coyotes (Canis latrans). J Wildl Dis 48: 717–723.
Liccioli S, Giraudoux P, Deplazes P, Massolo A. (2015): Wilderness in the ‘city’ revisited: different urbes shape transmission of Echinococcus multilocularis by altering predator and prey communities.Trends Parasitol 31: 297–305.
Mathis A, Deplazes P, Eckert J (1996): An improved test system for PCR-based specific detection of Echinococcus multilocularis eggs. J Helminthol 70: 219–222.
Mathy A, Hanosset R, Adant S, Losson B (2009): The carriage of larval Echinococcus multilocularis and other cestodes by the musk rat (Ondatra zibethicus) along the Ourthe River and its tributaries (Belgium). J Wildl Dis 45: 279–287.
McManus DP, Gray DJ, Zhang W, Yang Y (2012): Diagnosis, treatment, and management of echinococcosis. BMJ Clin Res Ed. 344: e3866.
Meyer A, Conraths FJ, Schneemann C, Wienrich V, Kershaw O, Gruber AD (2013): [Lethal alveolar echinococcosis in a dog: clinical symptoms and pathology]. Berl Munch Tierarztl Wochenschr 126: 408-414.
Miterpáková M, Antolová D, Ševčíková Z, Stanko M, Dinkel A, Gašpar V, Dubinský P (2006): Echinococcus multilocularis in musk rat (Ondatra zibethicus): the first finding of the parasite in naturally infected rodent in the Slovak Republic. Helminthologia 43: 76–80.
Oksanen A, Siles-Lucas M, Karamon J, Possenti A, Conraths FJ, Romig T, Wysocki P, Mannocci A, Mipatrini D, La Torre G, Boufana B, Casulli A (2016): The geographical distribution and prevalence of Echinococcus multilocularis in animals in the European Union and adjacent countries. A systematic review and meta-analysis. Parasit Vectors 9: 519.
Palmer SR (2011): Biology, clinical practice, and public health control. In: Palmer SR, Lord Soulsby, Torgerson P, Brown DWG (Eds.). Oxford textbook of zoonoses. Oxford University Press, Oxford.
Peregrine AS (2015): Alveolar echinococcosis in dogs: an emerging issue? Vet Rec 177: 567–568.
Peregrine AS, Jenkins EJ, Barnes B, Johnson S, Polley L, Barker IK, de Wolf B, Gottstein B (2012): Alveolar hydatid disease (Echinococcus multilocularis) in the liver of a Canadian dog in British Columbia, a newly endemic region. Can Vet J 53: 870–874.
Peters M, Kilwinski J, Wohlsein P, Conraths FJ (2010): Alveolar echinococcosis in a captive red-necked wallaby (Macropus rufogriseus). Berl Munch Tierarztl Wochenschr 123: 63–69.
Rehmann P, Gröne A, Gottstein B, Sager H, Müller N, Völlm J, Bacciarini LN (2005): Alveolar echinococcosis in the zoological garden Basle. Schweiz Arch Tierheilkd 147: 498–502.
Robert Koch Institut: RKI-Ratgeber Echinokokkose. https://www.rki.de/DE/Content/Infekt/EpidBull/Merkblaetter/Ratgeber_Ech… (accessed 08 February 2020).
Romig T, Ebi D, Wassermann M (2015): Taxonomy and molecular epidemiology of Echinococcus granulosus sensu lato. Vet Parasitol 213: 76–84.
Siles-Lucas M, Casulli A, Conraths FJ, Müller N (2017): Laboratory diagnosis of Echinococcus spp. in human patients and infected animals. Adv Parasitol 96: 159–257.
Sonnenburg J, Ryser-Degiorgis M-P, Kuiken T, Ferroglio E, Ulrich RG, Conraths FJ, Gortázar C, Staubach C (2017): Harmonizing methods for wildlife abundance estimation and pathogen detection in Europe-a questionnaire survey on three selected host-pathogen combinations. BMC Vet Res 13: 53.
Staubach C, Hoffmann L, Schmid VJ, Ziller M, Tackmann K, Conraths FJ (2011): Bayesian space-time analysis of Echinococcus multilocularis-infections in foxes. Vet Parasitol 179: 77–83.
Staubach C, Thulke HH, Tackmann K, Hugh-Jones M, Conraths FJ (2001): Geographic information system-aided analysis of factors associated with the spatial distribution of Echinococcus multilocularis infections of foxes. Am J Trop Med Hyg 65: 943–948.
Stojkovic M, Junghanss T (2013): Cystic and alveolar echinococcosis. Handb Clin Neurol 114: 327–334.
Tackmann K, Janitschke K (1996): Zur epidemiologischen Situation des Echinococcus multilocularis – breitet sich eine gefährliche Parasitose in der Bundesrepublik Deutschland aus? RKI Epid Bull 14: 123.
Tackmann K, Löschner U, Mix H, Staubach C, Thulke HH, Conraths FJ (1998): Spatial distribution patterns of Echinococcus multilocularis (Leuckart 1863) (Cestoda: Cyclophyllidea: Taeniidae) among red foxes in an endemic focus in Brandenburg, Germany. Epidemiol Infect 120: 101–109.
Tackmann K, Loschner U, Mix H, Staubach C, Thulke HH, Ziller M, Conraths FJ (2001): A field study to control Echinococcus multilocularis-infections of the red fox (Vulpes vulpes) in an endemic focus. Epidemiol Infect 127, 577–587.
Tackmann K, Mattis R, Conraths FJ (2006): Detection of Echinococcus multilocularis in foxes. Evaluation of a protocol of the intestinal scraping technique. J Vet Med B Infect Dis Vet Public Health 53, 395–398.
Thomas H, Gönnert R (1978): The efficacy of praziquantel against cestodes in cats, dogs and sheep. Res Vet Sci 24: 20–25.
Thomas MN, Zwingelberg S, Angele M, Guba M, Werner J (2017): Diagnosis and treatment of cystic and alveolar echinococcosis. MMW Fortschr Med 159: 38–42.
Thompson RC, Deplazes P, Eckert J (2003): Observations on the development of Echinococcus multilocularis in cats. J Parasitol 89: 1086–1088.
Thompson RCA (2017): Biology and Systematics of Echinococcus. Adv Parasitol 95, 65–109.
Torgerson PR (2003): The use of mathematical models to simulate control options for echinococcosis. Acta Trop 85: 211–221.
Torgerson PR, Budke CM (2003): Echinococcosis – an international public health challenge. Res Vet Sci 74: 191–202.
Torgerson PR, Schweiger A, Deplazes P, Pohar M, Reichen J, Ammann RW, Tarr PE, Halkic N, Müllhaupt B (2008): Alveolar echinococcosis: from a deadly disease to a well-controlled infection. Relative survival and economic analysis in Switzerland over the last 35 years. J Hepatol 49: 72–77.
Torgerson PR, Keller K, Magnotta M, Ragland N (2010): The global burden of alveolar echinococcosis. PLoS Negl Trop Dis 4: e722.
Trachsel D, Deplazes P, Mathis A (2007): Identification of taeniid eggs in the faeces from carnivores based on multiplex PCR using targets in mitochondrial DNA. Parasitology 134: 911–920.
Veit P, Bilger B, Schad V, Schafer J, Frank W, Lucius R (1995): Influence of environmental factors on the infectivity of Echinococcus multilocularis eggs. Parasitology 110 (Pt 1): 79–86.
Vuitton DA, Zhou H, Bresson-Hadni S, Wang Q, Piarroux M, Raoul F, Giraudoux P (2003): Epidemiology of alveolar echinococcosis with particular reference to China and Europe. Parasitology 127 (Suppl): S87–107.
Vuitton DA, Demonmerot F, Knapp J, Richou C, Grenouillet F, Chauchet A, Vuitton L, Bresson-Hadni S, Millon L (2015): Clinical epidemiology of human AE in Europe. Vet Parasitol 213: 110–120.
Wahlström H, Enemark H-L, Davidson RK, Oksanen A (2015): Present status, actions taken and future considerations due to the findings of E. multilocularis in two Scandinavian countries. Vet Parasitol 213: 172–181.
Wen H, Vuitton L, Tuxun T, Li J, Vuitton DA, Zhang W, McManus DP (2019): Echinococcosis: Advances in the 21st Century. Clin Microbiol Rev 32: e00075–18.
Weiss AT, Bauer C, Köhler K (2010): Canine alveolar echinococcosis: morphology and inflammatory response. J Comp Pathol 143: 233-238.
Woolsey ID, Bune NE, Jensen PM, Deplazes P, Kapel CM (2015a): Echinococcus multilocularis infection in the field vole (Microtus agrestis): an ecological model for studies on transmission dynamics. Parasitol Res 114: 1703–1709.
Woolsey ID, Jensen PM, Deplazes P, Kapel CM (2015b): Establishment and development of Echinococcus multilocularis metacestodes in the common vole (Microtus arvalis) after oral inoculation with parasite eggs. Parasitol Int 64: 571–575.
Woolsey ID, Jensen PM, Deplazes P, Kapel CM (2016): Peroral Echinococcus multilocularis egg inoculation in Myodes glareolus, Mesocricetus auratus and Mus musculus (CD-1 IGS and C57BL/6j). Int. J. Parasitol. Parasites Wildl 5: 158–163.
Zeyhle E, Abel M, Frank W (1990): Epidemiologische Untersuchungen zum Vorkommen von Echinococcus multilocularis bei End- und Zwischenwirten in der Bundesrepublik Deutschland. Mitt Osterr Ges Tropenmed Parasitol 12: 221–232.



Kostenfreier Download
Klicken Sie hier, wenn Sie das PDF BMTW-10.23760005-9366-2020-5-Conraths.pdf (0.4 MB) herunterladen möchten
Kostenfreier Download
Klicken Sie hier, wenn Sie das PDF BMTW-10.23760005-9366-2020-5-Connraths_Tabelle 1.pdf (0.13 MB) herunterladen möchten
Kostenfreier Download
Klicken Sie hier, wenn Sie das PDF BMTW-10.23760005-9366-2020-5-Connraths_Tabelle 2.pdf (0.12 MB) herunterladen möchten
Kostenfreier Download
Klicken Sie hier, wenn Sie das PDF BMTW-10.23760005-9366-2020-5-Connraths_Tabelle 3.pdf (0.12 MB) herunterladen möchten



{kind=link}
{kind=link}