
Vergleichende Aspekte der permanenten Tracheotomie bei Katzen und Kindern – können wir von der Kindermedizin lernen?
Kleintierpraxis 67, 372–385
DOI: 10.2377/0023-2076-67-372
© M. & H. Schaper GmbH. 2022
Publiziert: 07/2022
Summary
Permanent tracheostomy in cats is associated with a high rate of complications and mortality. The aim of this study was to compare surgical methods and post-operative care protocols for tracheostomy in cats and children. Therefore, a literature research was performed using online databases and common textbook chapters. Sixty-six publications were identified for this review. The results showed, that in many ways the feline and pediatric respiratory tract are very similar. However, the feline respiratory tract has significantly more respiratory glands, which extend further into the bronchioles. This increases the risk of excessive mucus secretion after tracheostomy. To date, precise anatomical dimensions of the feline trachea have not been documented. In pediatric medicine, surgical and postoperative treatment protocols for permanent tracheostomy are well researched, which keeps complication and mortality rates low. Only one surgical procedure for permanent tracheostomy of the feline patient has been described and no standardized postoperative guidelines exist. In order to establish and optimize surgical protocols for the cat, further studies of the feline tracheal dimensions are warranted. The effect of the alteration of mucosal glands with chronic irritation are needed to help reduce excessive mucus secretion. Standardized postoperative guidelines should be established for medical staff and owners.
Zusammenfassung
Die permanente Tracheostomie ist bei Katzen mit einer hohen Komplikations- und Sterblichkeitsrate verbunden. Ziel dieser Studie war es, chirurgische Methoden und postoperatives Management zwischen Katzen und Kindern zu vergleichen. Eine Literaturrecherche wurde anhand von Online-Datenbanken und anerkannten Buchkapiteln durchgeführt, 66 Publikationen konnten für die Studie genutzt werden. Die Ergebnisse zeigten, dass sich der Respirationstrakt von Katzen und Kindern in vielerlei Hinsicht sehr ähnelt. Auffällig war, dass bei Katzen eine signifikant größere Anzahl an submukosalen Drüsen vorhanden ist, die deutlich weiter in die Bronchiolen reichen und sich damit das Risiko einer auftretenden Hypersekretion nach durchgeführter Tracheostomie erhöhen kann. Darüber hinaus konnten im anatomischen Vergleich keine genauen Abmessungen über die Trachea der Katze gefunden werden. In der Pädiatrie existieren gut ausgearbeitete chirurgische und postoperative Protokolle, welche die Komplikations- und Sterblichkeitsraten gering halten. In der Veterinärmedizin ist nur ein chirurgisches Verfahren der permanenten Tracheostomie beschrieben und es gibt keine standardisierten postoperativen Protokolle für Katzen. Um chirurgische Protokolle und alternative Methoden entwickeln zu können, sind weitere Studien über die genaue Anatomie sowie die histologischen Veränderungen nach chronischer Reizung der Trachea notwendig, damit das Auftreten einer Hypersekretion verringert wird. Für medizinisches Personal und Besitzer können dann standardisierte postoperative Protokolle entwickelt werden.
Introduction
Permanent tracheostomy has become a routine clinical intervention in children (> 4000/y in the US) (Watters 2017, Muller et al. 2019, Esianor et al. 2020), but is a rare procedure in small animals (Guenther-Yenke and Rozanski 2007, Stepnik et al. 2009, Occhipinti and Hauptman 2014, Tobias and Johnston 2018, Grimes et al. 2019). Tracheostomy is a surgical procedure during which an opening is created in the ventral trachea in order to bypass an obstructed upper airway (Bluestone and Rosenfeld 2002, Hardie 2014, Aronson 2016, Clarke 2017, Tobias and Johnston 2018, Puri and Höllwarth 2019). Temporary tracheostomies are typically performed to facilitate respiratory ventilation in emergency cases of life-threatening upper airway obstruction or during surgeries where placement of an endotracheal tube is not possible. Permanent tracheostomy is performed in patients with progressive or permanent conditions, which cannot be treated successfully by other methods. The procedure involves the surgical creation of a stoma distal to the obstruction by either removing a segment of the tracheal wall and suturing tracheal mucosa to the skin or, in case of total laryngectomy, suturing the transected end of the trachea to the skin (Hedlund et al. 1982, Bluestone and Rosenfeld 2002, Clarke 2017, Tobias and Johnston 2018, Puri and Höllwarth 2019, Vincenti et al. 2021).
Tracheostomy and its management is considered a challenging procedure in cats due to a high complication and mortality rate (Guenther-Yenke and Rozanski 2007, Stepnik et al. 2009). In particular hypersecretions with formation of mucous plugs and stoma-related complications including localized tracheal collapse and stoma stricture can lead to death by asphyxiation (Guenther-Yenke and Rozanski 2007, Stepnik et al. 2009). Due to the high rate of complications and mortality, data regarding long-term outcomes of tracheostomized cats are extremely scarce (Guenther-Yenke und Rozanski 2007, Stepnik et al. 2009, Vincenti et al. 2021). There are no standardized postoperative management protocols for cats and recommendations vary greatly between practices (Stepnik et al. 2009). Already existing guidelines for artificial airway management are mostly based on experiences with dogs. Since the complications and outcomes in cats are different from dogs (aspiration pneumonia, skinfold occlusion and stoma stenosis), a comparison with dogs was not considered (Occhipinti and Hauptman 2014, Grimes et al. 2019). Other experimental animals were not taken into consideration, despite they are often used for animal model-based tracheostomies for medical training. For these species, long-term outcomes, complications and management are not adequately described as well as tracheal proportions are not suitable to that of the cat. On the other hand, in pediatric medicine, surgical techniques, postoperative care and caretaker instructions are substantially better developed and standardized.
Therefore, a comparison between the surgical techniques, postoperative care and management of permanent tracheostomies in cats and children was performed. Tracheal anatomy, histology and physiology were also compared. The aim of the present study was to discover if the information deriving from pediatric medicine could be potentially translated to the feline patient receiving a permanent tracheostomy.
Top Job:
Materials and methods
Literature research was performed online with PubMed, ScienceDirect, Researchgate, Sagepub and Google Scholar using the following key search terms: “tracheostomy”, “tracheotomy”, “trachea”, “tracheal histology/anatomy” and a term defining the relevant participants “cats/feline”, “small animals”, “children/pediatric”.
The focus of the search was surgical methods, complications associated with the procedure and management of tracheostomy. All possible combinations were used and each articles reference list was searched for additional relevant articles. No restrictions regarding publication date were applied but articles published between 2010 and 2022 were prioritized. Additional records were identified from common textbook chapters about anatomy, histology and physiology of the pediatric and feline trachea and the respiratory system.
A total of 298 articles were identified 66 of which met the inclusion criteria. Included literature was constituted by studies on tracheostomy, physiology/pathophysiology of the trachea and cytology/histology of the trachea in small animals, especially cats/felines. Given the limited amount of data available for tracheostomy in cats, all accessible articles were included. Due to a high number of studies from the field of human pediatric medicine, the latest research about tracheostomy techniques, post-operative management and complications associated with the procedure were selected. Retrospective, clinical and long-term studies were prioritized and studies that refer to earlier publications on anatomic, physiologic and surgical basics were included.
Results
Comparative anatomy of larynx and trachea in cats and human children ( Tab. 1)
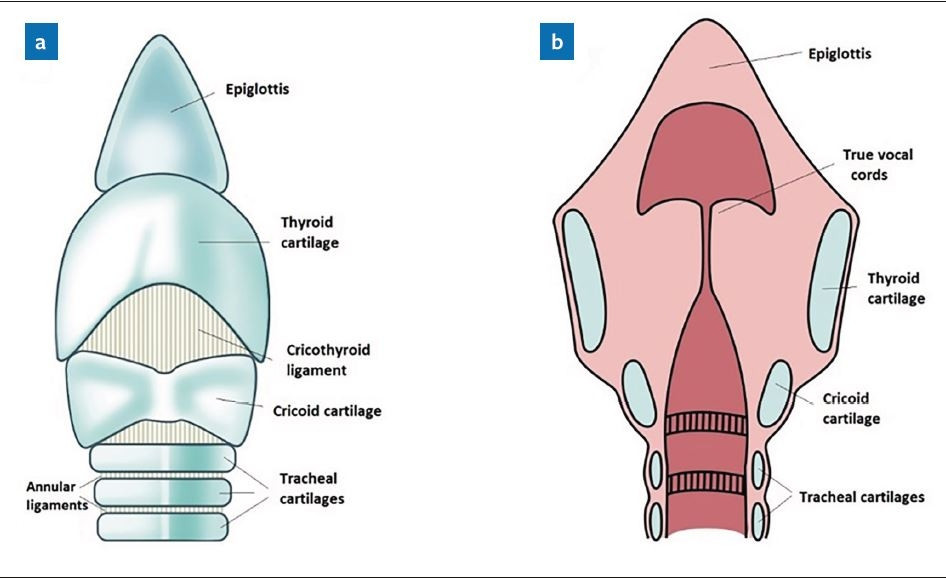
The larynx is composed of three unpaired bilateral cartilages (epiglottis, cricoid and thyroid) and one paired cartilage (arytenoids) (Nickel et al. 2004, König et al. 2007, Hudson and Hamilton 2010). The epiglottis of the feline larynx is spade-shaped (Hudson and Hamilton 2010). The hyoepiglottic muscle is connected to the ceratohyoid bone and is responsible for ventral movement of the epiglottis during breathing (Weissengruber et al. 2002). The arytenoid cartilages are small and the corniculate and cuneiform processes are absent. The arytenoid cartilages are pyramidal in shape and connected by an interarytenoid ligament (Hudson und Hamilton 2010). There are two pairs of tissue folds at the cranial end: the vestibular and the vocal cord folds (Kirby 2014). An absence of laryngeal ventricles has been described in the feline larynx (Fig. 1) (Ettinger and Feldman 2010, Hudson and Hamilton 2010).
The sides of the epiglottis are directly connected to the cricoid lamina by laryngeal mucosa (MacPhail 2014). The feline trachea measures 7–10 mm in diameter and the number of cartilage rings ranges from 38 to 43 (Nickel et al. 2004, König et al. 2007, Hudson and Hamilton 2010). In the current literature, the average length and exact position of the trachea relative to the spine could not be found.

The human epiglottis is generally leaf-shaped but 50% of children have an omega-shape appearance (Minnich and Mathisen 2007, Prakash and Johnny 2015). The epiglottis is equipped with a hyoepiglottic ligament rather than the hyoepiglottic muscle described in cats. As this ligament has no contractile function, the thyroepiglottic muscle acts as a depressor of the human epiglottis instead (Amis et al. 1998).
One crucial difference between the feline and human larynx is that humans have a vocal ligament for phonation and pitch control. The cricothyroid and thyroarytenoid muscles differ individually in mass cross-sectional area and fiber orientation to control the arytenoid position, vocal fold tension and vocal fold length (Döllinger et al. 2011). The child’s larynx, especially in children under two years of age, is located higher in the neck at the level of the C2–C3 vertebra and lies more ventrally (Griscom und Wohl 1986, Westhorpe 1987, Prakash und Johnny 2015). The arytenoids are prominent and the membranous portion of the vocal fold is short (Prakash and Johnny 2015). The caudal margin of the cricoid cartilage lies at the level of the C4 vertebra (Prakash and Johnny 2015). The laryngeal structures lower with increasing age (Griscom and Wohl 1986, Prakash and Johnny 2015). In children aged two to twelve, the larynx extends between the level of the C3 and C5 vertebra. In children older than 12, the cricoid cartilage is found at the level of C7 vertebra (Westhorpe 1987). The number of the C-shaped cartilaginous rings of the trachea ranges between 18 and 22 (Breatnach et al. 1984, Minnich and Mathisen 2007, Furlow and Mathisen 2018). Children aged 0–2 years have an average tracheal diameter of 5.3 mm and a mean tracheal length of 5.4 cm. In 2–4 years of age, the mean tracheal length is 6.4 cm, with a diameter of around 7.4 mm (Griscom and Wohl 1986, Prakash and Johnny 2015). By the time children reach 8–10 years of age, the trachea shows a mean diameter of 10.5 mm and a mean length of 8.8 cm (Griscom and Wohl 1986, Prakash and Johnny 2015) (Tab. 1).
Histology of the respiratory tract wall (Tab. 2)
The histologic composition is similar between species despite that variations in the frequency may occur in each cell type/tissue and location (Premanandan and Jennings 2017, Whitsett 2018). The respiratory tract is lined with the same tissue found in the nose, larynx, trachea and bronchi (Premanandan and Jennings 2017, Whitsett 2018). The mucosa comprises a pseudostratified columnar epithelium containing ciliary epithelium, non-ciliary epithelium and secretory cells, which cause an upward stream of mucus and foreign bodies (Jeffery 1978, Wine and Joo 2004, Widdicombe and Wine 2015, Premanandan and Jennings 2017). More distal parts of the airways have smaller and fewer secretory cells than proximal parts. Submucosal glands with included mucous and serous cells, non-ciliated club cells and epithelial goblet cells represent the three most common secretory cell types of the respiratory epithelium (Whitsett 2018). Of these, the mucus-producing goblet cells occur frequently and are filled with mucin, a viscous substance with a high molecular weight. The submucosal glands occupy a significant proportion of the tracheal and bronchial wall and contain seromucous secretions (Jeffery 1978, Ballard and Inglis 2004, Widdicombe and Wine 2015, Premanandan and Jennings 2017, Whitsett 2018). Club cells (previously known as Clara cells) continuously release gel-forming mucin and have stem cell capability. In response to irritation, club cells are able to convert into goblet cells (Widdicombe and Wine 2015).
When faced with chronic irritation, as is the case after tracheostomy, the secretory glands of the respiratory epithelium can undergo different modifications (Nadel 2013). To protect the airways from infection or foreign bodies, the submucosal glands react with hypertrophy and hyperplasia, goblet cells mostly undergo hyperplasia and club cells are able to convert into goblet cells (Jeffery 1978, Widdicombe and Wine 2015). All these modifications result in increased secretion, particularly mucous secretion. Prolonged exposure of the epithelium to irritants can cause hypersecretion (Nadel 2013).
The submucosal glands are innervated by parasympathetic (cholinergic), sympathetic (adrenergic) and sensory-efferent nerves. Mucous glands are stimulated by beta (β)-adrenergic receptor agonists, while serous glands are stimulated by alpha(α)-adrenergic receptor agonists (Gallagher et al. 1975, Rogers 2001). The adrenergic stimulation varies between species; alpha(α)-adrenergic receptor agonists exert a strong effect in cats but have little or no effect on human glands (Ballard and Inglis 2004). The number and size of the glands also differ between species. While the glands are found in the tertiary bronchi and proximal bronchioles in cats, they are limited to the upper respiratory tract, primary and secondary bronchi in humans (Jeffery 1978, Premanandan and Jennings 2017, Whitsett 2018). In the feline trachea, submucosal glands constitute between 61% and 94% of the total secretory cell volume with 40–80% of them belonging to the serous category (Gallagher et al. 1975, Arara 2011). The submucosal glands are particularly abundant in the trachea and bronchi of cats than in any other species. The goblet cells constitute between 7% and 15% of all epithelial cells of the respiratory tract in cats and are frequently found deep in the lung (Jeffery 1978). Club cells are the predominant secretory cells of the respiratory bronchioles (Gallagher et al. 1975, Widdicombe and Wine 2015). In the human trachea, the cell volume of the submucosal glands consists of 40% mucous and 60% serous cells (Wine und Joo 2004).
Reid Index
The Reid index is defined as the ratio of the mean thickness of the submucosal mucous secreting glands/ thickness of the bronchial wall of the respiratory tract (Arara 2011). The Reid index value in healthy cats is higher than in healthy humans and ranges between 0.61 and 0.65. The feline bronchial glands are histologically more prominent than in other domestic animals and humans (Arara 2011). The Reid Index in healthy adult humans should be smaller than 0.4. In patients with chronic bronchitis, which causes submucosal gland hypertrophy and hyperplasia, the Reid Index rises to 0.5 or higher. The Reid Index is age-dependent, the physiological ratios in healthy infants with 0.37 and 0.41 are higher than in adults (Ballard and Inglis 2004)
Tracheostomy
The most common indications for permanent tracheostomy differ between species. The most common reasons for permanent tracheostomy in cats include laryngeal masses, inflammatory laryngeal diseases, laryngeal paralysis and trauma (Stepnik et al. 2009, Tobias and Johnston 2018). Indications for pediatric tracheostomy include upper airway obstruction secondary to infectious disorders as well as respiratory, cardiopulmonary or neurological impairment, resulting in the need for prolonged ventilation support (Gergin et al. 2016).
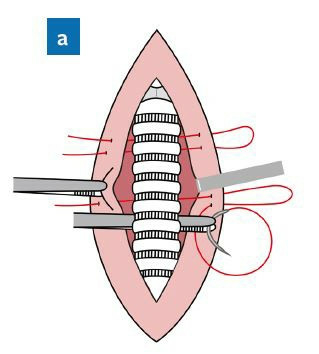
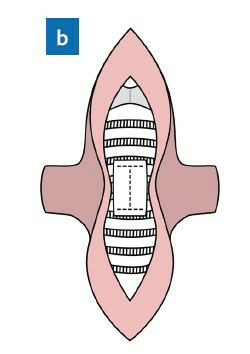
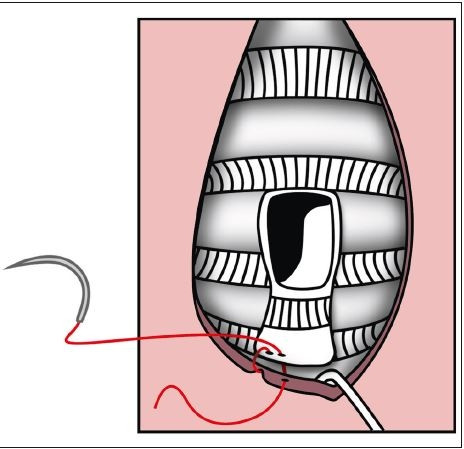
The literature search revealed only one surgical method for permanent tracheostomy in cats, which is adapted from dogs (Hedlund 1994, Hardie 2014, Aronson 2016, Tobias and Johnston 2018). Tracheostomy is performed under general anesthesia. The cat is positioned in dorsal recumbency, the neck is extended and surgically prepared. The incision is made caudal to the location of the obstruction. The skin incision is made on the ventral midline of the trachea, spanning from the cricoid cartilage to the 6th tracheal ring (Hedlund 1994, Aronson 2016, Tobias and Johnston 2018). Due to a higher incidence of complications, incisions caudal to the 12th tracheal ring are not recommended (Tobias and Johnston 2018). Excessive kinking of the trachea in that region may result in a higher mortality rate secondary to airway obstruction (Tobias and Johnston 2018). Mattress sutures can then be used to appose the previously separated sternohyoid muscles at the dorsal midline of the trachea (Fig. 2a). This moves the trachea in a ventral direction and thus reduces tension on the stoma (Tobias und Johnston 2018). The tracheal stoma is created by removing a rectangular segment (1/3–1/2 of the circumference of the trachea in width) from the ventral aspect of 3 to 5 tracheal rings (Fig. 2b) (Hedlund 1994, Bartoli et al. 2008, Aronson 2016, Tobias and Johnston 2018). A section of the skin, similar to the size of the stoma is resected to form the final opening (Fig. 2b). If excess folds of skin pose a risk of obstruction, a larger section can be resected. In order to prevent tracheal collapse, the tracheal stoma should be kept as small as possible (Hedlund 1994). However, tissue contraction during the healing phase can cause a significant reduction of the stoma and should be taken into consideration (Hedlund et al. 1982, Hedlund 1994, Hardie 2014, Tobias and Johnston 2018). Unfortunately, no species-specific recommendations regarding stoma size currently exist. An H-shaped incision of the tracheal mucosa ensues. The resulting flaps of mucosa are folded over the edges of the tracheal cartilages and anastomosed to the skin (Fig. 2c) (Hedlund 1994, Aronson 2016).
Tracheostomies are typically performed under general anesthesia with the patient‘s head stabilized and neck extended using a shoulder roll. It is important not to overextend the neck as this can cause a pull of thoracic vessels into the neck (Clarke 2017). To minimize bleeding, a local anesthetic and a vasoconstrictor are used. The transverse skin incision is made halfway between the cricoid cartilage and the suprasternal notch. The subcutaneous fat is removed, and the strap muscles are separated along the midline raphe. If the thyroid isthmus be positioned across the trachea, it can be retracted cranially if possible or severed using ligation or bipolar diathermy (Bluestone and Rosenfeld 2002, Clarke 2017, Puri and Höllwarth 2019). A vertical incision across two tracheal rings is then made in the midline of the tracheal wall between the second and fourth tracheal ring. Since no cartilage is removed in pediatric tracheostomy (Bluestone and Rosenfeld 2002) and the tracheal stoma can close quickly without a tracheostomy tube in place, silicone or silastic tracheostomy tubes are necessary for both temporary and permanent tracheostomy techniques. Tracheostomy tubes come in different sizes and, in children aged under one year, should be chosen according to the following formula: (age in years/4) + 4mm = internal diameter of the tube (Watters 2017). Given the strong foreign body inflammatory reactions seen in children, pediatric tracheostomy tubes have a small diameter without an inner cannula (single lumen cannulas), have no fenestration and are uncuffed. The particularly thin walls of the tube leave room for a larger lumen with minimal friction to the skin of the neck resulting in lower inflammatory response (Bluestone and Rosenfeld 2002, Clarke 2017). After tube placement, maturation sutures can be used to fasten the edges of the tracheal wall to the skin. This facilitates the development of a safe stoma and prevents accidental decannulation and formation of granulation tissue (Craig et al. 2005, Watters 2017).
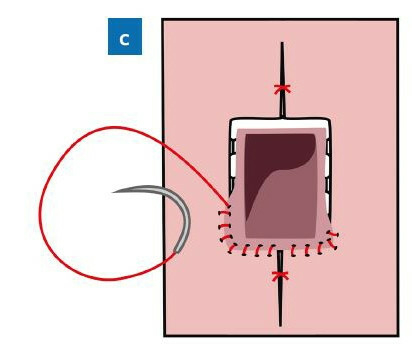
This technique was developed to reduce the incidence of major complications such as accidental decannulation and pneumothorax. Instead of a transverse incision, an X-shaped skin incision is made between the sternal notch and the cricoid cartilage. The resulting skin flaps are circumferentially undermined, muscles and thyroid isthmus are separated as described above. A cross-shaped incision is used to gain access to the trachea. The triangular skin flaps are circumferentially aligned with the triangular tracheal flaps to create the final stoma (Fig. 3) (Koltai 1998, Solares et al. 2004, Schwarz et al. 2017, Thurnher 2020).
Due to the attachment of the trachea to the skin, in the event of accidental decannulation the tube can easily be replaced (Schwarz et al. 2017). This method is therefore considered an advantageous alternative for patients with a low probability of a permanent future decannulation (Schwarz et al. 2017).

Depending on the underlying indication, an array of other surgical techniques can be utilized to optimize the outcome. One example is the inverted U-shaped “Björk flap”, typically used in adults for long-term tracheostomies, in which a tracheal flap is attached to the skin to create a potentially larger stoma than in other techniques (Fig. 4) (Kennedy et al. 2021). This technique is less common in the pediatric medicine and only used in older children with adequate tracheal width (D’Souza et al. 2016, Watters 2017, Fliss 2021). Another option, known as tracheal window resection involves the excision of a square-shaped of the tracheal rings without tracheal flaps and is also used in veterinary medicine (Scurry and McGinn 2007, Cipriano et al. 2015, Janik et al. 2018). These techniques are not usually used in pediatric medicine primarily due to the limited space and the chances of injury of adjacent structures.
Postoperative care
In cats, intensive care and close observation in an intensive care unit (ICU) is necessary in the postoperative period to prevent life-threatening complications (Guenther-Yenke und Rozanski 2007, Stepnik et al. 2009, Tobias and Johnston 2018, Vincenti et al. 2021). Intensive care should be performed for at least two weeks in the ICU with close observation of mucous secretions until the stoma is healed and secretions decrease (Tobias and Johnston 2018, Vincenti et al. 2021). In these 14 days after surgery, the tracheal mucosa undergoes squamous metaplasia with possible excessive mucus production (Hedlund et al. 1982, Tobias and Johnston 2018, Vincenti et al. 2021). In this period, emergency equipment, oxygen supply and material for cleaning and suctioning must be readily available at all times (Aronson 2016, Tobias and Johnston 2018). The stoma must be cleaned, humidified and suctioned at least every four to six hours. Humidification is important to decrease mucus production and should be performed equally regularly (Aronson 2016, Tobias and Johnston 2018). Some authors also recommend applying a thin layer of antibiotic ointment to protect the skin from secretions surrounding the stoma (Aronson 2016, Tobias and Johnston 2018). In dogs, it has been shown that the tracheal epithelium reaches a relatively normal state after 16 weeks (Hedlund et al. 1982). While there is no specific data regarding tracheal re-epithelialization in cats, a similar time frame is to be expected. Before discharging feline tracheostomy patients, owners must receive adequate instructions on cleaning the stoma and suctioning the trachea using a catheter and syringe (Vincenti et al. 2021). Secretions slowly decrease over time but can still cause obstruction in the following weeks. To prevent obstruction, close observation, suctioning, humidification and cleaning of the stoma site should be continued in homecare over 4–8 weeks until secretions decrease dramatically (Hardie 2014, Tobias and Johnston 2018).
Tracheostomy tubes are used for temporary tracheostomy in small animals (Mann and Flanders 2012, Aronson 2016, Tobias and Johnston 2018). There are several types of tubes, with single or double cannulas, cuffed and uncuffed. The double cannula has an inner cannula that can be removed, leaving the outer cannula in the trachea. For cleaning, the inner cannula can easily be removed and cleaned separately. The single cannula is more difficult to clean; the entire tracheostomy tube must be replaced if it cannot be cleaned effectively (Mann and Flanders 2012, Aronson 2016, Tobias and Johnston 2018).
The tube has to be inspected at least every two to four hours (Mann and Flanders 2012, Tobias and Johnston 2018). Patients producing excessive secretions may require care every 30 minutes or more often (Sierra and King 2012). The tube should be inspected for debris and accumulated secretions that can be removed with sterile pipe cleaners or a moistened sterile cotton swab. Additionally, auscultation should be done as frequently as necessary to detect diminished air movement, wheezing or whistling sounds (Sierra and King 2012). If secretion accumulation appears distal of the tube, suctioning is necessary before tube obstruction occurs. To ensure oxygen saturation, patients should be preoxygenated for five to ten minutes before suctioning (Sierra and King 2012, Tobias and Johnston 2018). The suction should be applied no longer than five seconds with a suction catheter and only a few centimeters past the end of the tube to prevent damage of the trachea (Sierra and King 2012). Direct instillation of sterile saline into to the tube is discussed to be less helpful as it can cause increased infections and further insult to the airway (Sierra and King 2012). Nebulization is recommended as a more effective way of humidification and moistening secretions (Sierra and King 2012).
After the surgery, the patient is monitored in an ICU for a minimum of five to seven days (Puri und Höllwarth 2019). Emergency equipment, including different sizes of tracheostomy tubes should be readily available. Regular cleaning of the tube and stoma is essential to prevent infection and obstruction. Suctioning of the tube is important to clear airway secretions. To avoid damage of the trachea, suctioning of the tube is only performed when necessary to remove excessive secretions and prevent obstruction (Nawrocki et al. 2021). Instillation of sterile saline before suctioning is no longer recommended due to a possible adverse effect on oxygen saturation (Nawrocki et al. 2021). In the immediate postoperative period, it is recommended to use an active heated humidity system. Active humidification devices use a heated humidifier with or without ventilator support (Volsko et al. 2021). Passive humidification should be continued using a heat and moisture exchanger (HME) that sits permanently on top of the tube (Birk et al. 2017, Puri and Höllwarth 2019). A HME should not be used when secretions are thick (risk of airway obstruction), a large leak around the tube is present or the patient cannot tolerate the additional dead space (Volsko et al. 2021). Recommendations about active warming and humidification of air exist for the care of a tracheostomized child with an inspired air temperature of 32–34 °C and humidity of 36–40 mg H₂O/L. In a study, a reduction in lower respiratory tract infection, tube obstruction and emergency tube change was achieved with long-term use (ten weeks) of active humidification at night and a HME during the day (McNamara et al. 2014). Inadequate humidification (< 25mg H₂O/L for 1 h or < 30mg H₂O/L for 24 h) has been reported to cause mucosal malfunction (Volsko et al. 2021). To keep the airway hydrated and humidified, an adequate water intake and infusions are necessary considering the greater fluid loss due to the tracheostomy (Avelino et al. 2017).
Daily cleaning of the tracheostomy site and frequent changing of moisture-wicking material that is placed under the tracheostomy tube if necessary is recommended for at least one week (Avelino et al. 2017, Volsko et al. 2021). A routine use of ointments is not recommended except in the presence of inflammation of the peristomal skin (Avelino et al. 2017). The first tracheostomy tube change is performed by healthcare staff between three to ten days and stay sutures are removed when the tracheostomy tract is fully healed (Bluestone and Rosenfeld 2002, Puri and Höllwarth 2019, Volsko et al. 2021). Tracheostomy tubes should be changed regularly at a minimum of every one to two weeks and as needed secondary to obstruction (Volsko et al. 2021). To standardize tracheostomy care, many facilities use a daily care bundle. The bundle contains components to assess tracheostomy cuff pressures (if inflated), provide humidification, ensure patency of the tube, conduct equipment safety checks, change of tracheostomy dressings and document the respiratory care plan (Volsko et al. 2021). Parents or caregivers must receive a detailed training program on tracheostomy management before the patient is discharged (Puri and Höllwarth 2019).
Complications
The complication and mortality rates in cats with permanent tracheostomy are high. Two retrospective studies found that the mean survival time of cats with permanent tracheostomies ranges from 20.5 to 42 days with 46% of cats dying shortly after the procedure due to post-operative complications (Guenther-Yenke and Rozanski 2007, Stepnik et al. 2009). In one report of a cat undergoing a permanent tracheostomy following a total laryngectomy, the cat was still alive 13 months after surgery (Vincenti et al. 2021). The most common complications include mucous plug formation with subsequent stoma or airway obstruction and dyspnea (14 out of 21 cats [Stepnik et al. 2009]) or death by asphyxiation (11 out of 21 cats (Stepnik et al. 2009) and two out of five cats (Guenther-Yenke and Rozanski 2007). Local tracheal collapse, stoma stricture, pulmonary edema and pneumonia, surgery site swelling, vomiting and anorexia/dysphagia have also been described (Guenther-Yenke and Rozanski 2007, Stepnik et al. 2009, Vincenti et al. 2021). Cats with a history of airway inflammation tend to show a significantly increased mucus production and epithelial irritation, according to one study (Stepnik et al. 2009). The mortality rate in these cats was 6.61 times as likely as in cats without any history of inflammatory laryngeal disease (Stepnik et al. 2009).
The mortality rate in tracheostomized children and infants (under two years of age) is reported at 8% and 23.5% respectively (Watters 2017, Esianor et al. 2020). However, major complications of the procedure are rare and the majority of deaths is linked to the initial cause of hospitalization (Watters 2017, Esianor et al. 2020). According to recent studies, better knowledge of the anatomy of the infant’s neck as well as better surgical routines have rendered perioperative complications such as accidental damage to the surrounding structures (esophagus, recurrent laryngeal nerve, brachiocephalic vein), major bleeding and pneumothorax/pneumomediastinum a rarity (Puri und Höllwarth 2019). Due to improved surgical techniques, intensive care and the creation of new medications, complication and mortality rates associated with the tracheostomy in the last three decades have decreased significantly (Dal’Astra et al. 2017, Lubianca Neto et al. 2020). In the immediate postoperative period, late hemorrhage of the trachea or surrounding structures, tracheal obstruction by secretions, tube dislodgement, accidental decannulation and surgical emphysema are the most common life threatening complications (Thompson et al. 2012). Obstruction of the trachea and accidental decannulation are among the most common late postoperative and homecare complications. As a long-term complication, persistent granulation tissue induced by chronic irritation and repeated suctioning has been reported. Granulation tissue growing into the tip of the cannula can induce airway obstruction and bleeding. Local infection is uncommon and antimicrobial treatment is successful in most cases. After decannulation, tracheal fistulas occur in 20–40% of cases and require revision surgery. Overall tracheostomy-related complications are experienced by 15%–20% of patients in recent studies (Berry et al. 2009, Watters et al. 2016, Watters 2017).
Discussion
On an anatomical level, the feline larynx and trachea are very similar to those of children. The adult feline trachea has a diameter of 7–10 mm (Hardie 2014) which is comparable to the tracheal diameter seen in children aged 2–10 years (7.4 mm–10.5 mm) (Griscom und Wohl 1986). Pediatric tracheostomy protocols thus appear to provide a good basis for the development of recommendations for performing the procedure in cats. However, exact data regarding the length and in situ positioning of the feline trachea are still lacking. In addition, data about the healing and adaptation process of the tracheal epithelium in cats were not reported and further anatomical and clinical studies are needed.
Only one surgical technique in cats has been investigated so far. It is plausible that adaptation of the surgical technique to the feline tracheal anatomy may reduce the rate of complications and improve the poor prognosis. For example, the creation of custom-made long-term tracheal tubes may also be beneficial to help the initial healing phase in cats and preventing tracheostomy stenosis or collapse.
A variety of surgical techniques for permanent tracheostomy in children has been developed to ensure the best results and comfort for the patient. A series of long-term studies and high case numbers have shown the concomitant improvements regarding outcome and prognosis (Puri and Höllwarth 2019, Esianor et al. 2020, Lubianca Neto et al. 2020).
Accidental premature decannulation poses a risk in both felines and children. Tracheal tubes that are frequently used and well accepted by children have the potential to show promising results in cats as well. Due to high secretions in cats, a tube tracheostomy should be done with double cannula tubes, that the inner cannula can be easily changed as they could get obstructed.
Histologically, cats have a significantly higher number of respiratory glands than humans, which extend much further into the bronchioles. This is associated with higher mucus production as a response to chronic irritation, which, in turn, increases the risk of airway obstruction. Given the increased risk of hypersecretion following chronic tracheal irritation, humidification of the inhaled air is of particular importance in the feline patient. The current standard in veterinary medicine is the use of nebulization to moisten the tracheal epithelium a few times a day. In children, permanent humidification of the tracheostomy tube is performed using active humidification and a HME attached to the top of the tube (Birk et al. 2017, Puri and Höllwarth 2019). This may present a promising alternative in the feline patient.
Notably, the feline adrenergic receptors of the secretory glands are stimulated differently than those of humans. Further research regarding the histologic response to chronic tracheal irritation and the medicinal reduction of excessive secretions of the mucosal glands in the cat can additionally help to reduce the risk of complications and death following permanent tracheostomy.
In one case report, a long-term intensive care immediately after the procedure and after hospital discharge had a positive outcome in a cat undergoing permanent tracheostomy after total laryngectomy (Vincenti et al. 2021). Unfortunately, to date, no standardized discharge instructions for owners of feline patients have been described. A better understanding of the feline tracheal dimensions could allow to consider alternative surgical techniques for feline permanent tracheostomy.
Over the past two decades, standardized surgical and postoperative protocols for permanent tracheostomy in children have improved (Dal’Astra et al. 2017, Lubianca Neto et al. 2020). Before pediatric patients are discharged from the hospital, parents or caretakers must undergo intensive training in postoperative tracheostomy management. This is associated with significantly fewer complications and a better long-term prognosis (Dal’Astra et al. 2017, Puri und Höllwarth 2019, Lubianca Neto et al. 2020).
The development of standardized postoperative guidelines and detailed training protocols for medical personnel and owners could pave the way to fewer complications and a longer life expectancy in feline tracheostomy patients.
Conclusions
Pediatric tracheostomy management appear to provide a promising basis for the development of protocols in the cat. Interestingly, data regarding precise anatomical dimensions of the feline trachea turned out to be extremely scarce. Furthermore, exact reports of the response to chronic irritation were not found. To reduce the high rate of complications and mortality in feline permanent tracheostomy patients, further anatomical and clinical studies are necessary. A modified surgical technique such as the Björk flap could be an option to extend the tracheal stoma and therefore reduce the onset of life-threatening complications. Postoperative guidelines for medical staff and owners may then be adapted to the feline patient to achieve a significantly better outcome.
Acknowledgments
The authors would like to thank Moritz Zimmermann for his friendly support and the design of all the graphics in the manuscript.
Conflict of interest
There are no protected, financial, professional or other personal interests in a product, service and/or company that could influence the content or opinions expressed in the manuscript. In case of possible conflict of interest it has to be indicated clearly.
Funding
The authors declare that they had no financial support for this publication.
Ethical approval
Authors assure to have met common international ethical guidelines during the genesis of the work, the underlying research and its publication. Informed consent: This work did not involve the use of animals and therefore informed consent was not required. No animals or humans are identifiable within this publication, and therefore additional informed consent for publication was not required.
Authors contribution
Conception/design of the work: SV.
Data collection: JZ.
Data analysis and interpretation: JZ.
Drafting the article: JZ.
Critical revision of the article: SV, JZ.
Final approval: SV, JZ.
Address for correspondence
Dr. Simona Vincenti, simona.vincenti@vetsuisse.unibe.ch
References
Literatur
Amis TC, O‘Neill N, Somma ED, Wheatley JR (1998): Epiglottic movements during breathing in humans. J Physiol 512(Pt 1): 307–314.
Arara A (2011): The Reid Index in Healthy Cats. Charlottetown, PE, University of Prince Edward Island.
Aronson LR (ed.) (2016): Upper Airway Disease: Tracheostomy. In: Small Animal Surgical Emergencies. Wiley Blackwell, Ames, Iowa, 261–269.
Avelino MAG, Maunsell R, Valera FCP, Lubianca Neto JF, Schweiger C, Miura CS, Chen VG, Manrique D, Oliveira R, Gavazzoni F, Picinin IFM, Bittencourt P, Camargos P, Peixoto F, Brandao MB, Sih TM, Anselmo-Lima WT (2017): First Clinical Consensus and National Recommendations on Tracheostomized Children of the Brazilian Academy of Pediatric Otorhinolaryngology (ABOPe) and Brazilian Society of Pediatrics (SBP). Braz J Otorhinolaryngol 83(5): 498–506.
Ballard ST, Inglis SK (2004): Liquid secretion properties of airway submucosal glands. J Physiol 556(Pt 1): 1–10.
Bartoli CR, Akiyama I, Okabe K, Diaz EA, Godleski JJ (2008): Permanent tracheostomy for long-term respiratory studies. J Surg Res 145(1): 124–129.
Berry JG, Graham DA, Graham RJ, Zhou J, Putney HL, O‘Brien JE, Roberson DW, Goldmann DA (2009): Predictors of clinical outcomes and hospital resource use of children after tracheotomy. Pediatrics 124(2): 563–572.
Birk R, Handel A, Wenzel A, Kramer B, Aderhold C, Hormann K, Stuck BA, Sommer JU (2017): Heated air humidification versus cold air nebulization in newly tracheostomized patients. Head Neck 39(12): 2481–2487.
Bluestone CD, Rosenfeld RM (2002): Tracheotomy. Surgical atlas of pediatric otolaryngology. BC Decker Inc, Hamilton, Hoboken, 585–596.
Breatnach E, Abbott GC, Fraser RG (1984): Dimensions of the normal human trachea. Am J Roentgenol 142(5): 903–906.
Cipriano A, Mao ML, Hon HH, Vazquez D, Stawicki SP, Sharpe RP, Evans DC (2015): An overview of complications associated with open and percutaneous tracheostomy procedures. Int J Crit Illn Inj Sci 5(3): 179–188.
Clarke RW (ed.) (2017): Tracheostomy. In: Pediatric Otolaryngology: Practical Clinical Management. Thieme, Stuttgart, 321–330.
Craig MF, Bajaj Y, Hartley BEJ (2005): Maturation sutures for the paediatric tracheostomy – an extra safety measure. J Laryngol Otol 119(12): 985–987.
D’Souza JN, Levi JR, Park D, Shah UK (2016): Complications Following Pediatric Tracheotomy. JAMA Otolaryngol Head Neck Surg 142(5): 484–488.
Dal’Astra A, Quirino A, Caixeta J, Gomes Avelino M (2017): Tracheostomy in childhood: Review of the literature on complications and mortality over the last three decades. Braz J Otorhinolaryngol 83(2): 207–214.
Döllinger M, Kobler J, Berry DA, Mehta DD, Luegmair G, Bohr C (2011): Experiments on Analysing Voice Production: Excised (Human, Animal) and In Vivo (Animal) Approaches. Curr Bioinform 6(3): 286–304.
Esianor BI, Jiang ZY, Diggs P, Yuksel S, Roy S, Huang Z (2020): Pediatric tracheostomies in patients less than 2 years of age: Analysis of complications and long-term follow-up. Am J Otolaryngol 41(2): 102368.
Ettinger SJ, Feldman EC (2010): Textbook of Veterinary Internal Medicine. Expert Consult. 7th. Saunders, Philadelphia, London, 1041.
Fliss DM (2021): 42 Pediatric Tracheostomy. In: Fliss DM, DeRowe A (eds.), Atlas of Pediatric Head and Neck and Skull Base Surgery. Thieme, Stuttgart.
Furlow PW, Mathisen DJ (2018): Surgical anatomy of the trachea. Ann Cardiothorac Surg 7(2): 255–260.
Gallagher JT, Kent PW, Passatore M, Phipps RJ, Richardson PS (1975): The composition of tracheal mucus and the nervous control of its secretion in the cat. Proc R Soc Lond B Biol Sci 192(1106): 49–76.
Gergin O, Adil EA, Kawai K, Watters K, Moritz E, Rahbar R (2016): Indications of pediatric tracheostomy over the last 30 years: Has anything changed? Int J Pediatr Otorhinolaryngol 87: 144–147.
Grimes JA, Davis AM, Wallace ML, Sterman AA, Thieman-Mankin KM, Lin S, Scharf VF, Hlusko KC, Matz BM, Cornell KK, Vetter CAM, Schmiedt CW (2019): Long-term outcome and risk factors associated with death or the need for revision surgery in dogs with permanent tracheostomies. J Am Vet Med Assoc 254(9): 1086–1093.
Griscom NT, Wohl ME (1986): Dimensions of the growing trachea related to age and gender. Am J Roentgenol 146(2): 233–237.
Guenther-Yenke CL, Rozanski EA (2007): Tracheostomy in cats: 23 cases (1998–2006). J Feline Med Surg 9(6): 451–457.
Hardie E (2014): Chapter 46 – Trachea and bronchus. In: Langley-Hobbs SJ, Demetriou JL, Ladlow JF (eds.), Feline Soft Tissue and General Surgery. Saunders Elsevier, St. Louis, 531–540.
Hedlund CS (1994): Tracheostomies in the management of canine and feline upper respiratory disease. Vet Clin North Am Small Anim Pract 24(5): 873–886.
Hedlund C, Tangner C, Montgomery D, Hobson H (1982): A Procedure for Permanent Tracheostomy and Its Effects on Tracheal Mucosa. Vet Surg 11(1): 13–17.
Hudson LC, Hamilton WP (2010): Atlas of feline anatomy for veterinarians. Teton NewMedia, Jackson, WY.
Janik S, Kliman J, Hacker P, Erovic BM (2018): Preserving the thyroidal isthmus during low tracheostomy with creation of a Bjork flap. Laryngoscope 128(12): 2783–2789.
Jeffery PK (1978): Structure and function of mucus-secreting cells of cat and goose airway epithelium. Ciba Found Symp (54): 5–23.
Kennedy M, Abdel-Aty Y, Lott D (2021): Comparing tracheostomy techniques: Bjork flap vs. tracheal window. Am J Otolaryngol 42(6): 103030.
Kirby B (2014): Chapter 52 – Larynx. In: Langley-Hobbs SJ, Demetriou JL, Ladlow JF (eds.), Feline Soft Tissue and General Surgery. Saunders Elsevier, St. Louis, 635–644.
Koltai PJ (1998): Starplasty: a new technique of pediatric tracheotomy. Arch Otolaryngol Head Neck Surg 124(10): 1105–1111.
König HE, Liebich HG (eds.) (2007): Veterinary Anatomy of Domestic Mammals: Textbook and Colour Atlas. 3rd ed. Schattauer, Stuttgart.
Lubianca Neto JF, Castagno OC, Schuster AK (2020): Complications of tracheostomy in children: a systematic review. Braz J Otorhinolaryngol: S1808-8694(20)30247-0.
MacPhail C (2014): Laryngeal Disease in Dogs and Cats. Vet Clin North Am Small Anim Pract 44(1): 19–31.
Mann FA, Flanders MM (2012): Temporary Tracheostomy. In: Burkitt Creedon JM, Davis H (eds.), Advanced Monitoring and Procedures for Small Animal Emergency and Critical Care. Wiley-Blackwell, Ames, Iowa, 306–317.
McNamara D, Asher M, Rubin B, Stewart A, Byrnes C (2014): Heated humidification improves clinical outcomes, compared to a heat and moisture exchanger in children with tracheostomies. Respir Care 59(1): 46–53.
Minnich DJ, Mathisen DJ (2007): Anatomy of the Trachea, Carina, and Bronchi. Thorac Surg Clin 17(4): 571–585.
Muller RG, Mamidala MP, Smith SH, Smith A, Sheyn A (2019): Incidence, Epidemiology, and Outcomes of Pediatric Tracheostomy in the United States from 2000 to 2012. Otolaryngol Head Neck Surg 160(2): 332–338.
Nadel JA (2013): Mucous hypersecretion and relationship to cough. Pulm Pharmacol Ther 26(5): 510–513.
Nawrocki P, Hughart J, Morgenstern J, Kaide CG (2021): Tracheostomy Emergencies. Emerg Med Rep 42(12).
Nickel R, Schummer A, Seiferle E, Habermehl KH, Frewein J (2004): Atmungsapparat. In: Nickel R, Schummer A, Seiferle E (Hrsg.), Lehrbuch der Anatomie der Haustiere. Band II. Parey, Stuttgart, 251 ff.
Occhipinti LL, Hauptman JG (2014): Long-term outcome of permanent tracheostomies in dogs: 21 cases (2000–2012). Can Vet J 55(4): 357–360.
Prakash M, Johnny JC (2015): Whats special in a child‘s larynx? J Pharm Bioallied Sci 7(Suppl 1): 55–58.
Premanandan C, Jennings R (eds.) (2017): Chapter 10: Respiratory System. In: Veterinary Histology. State University Libraries, Ohio, 159–171.
Puri P, Höllwarth ME (eds.) (2019): Tracheostomy in Infants. In: Pediatric Surgery. 2nd ed. Springer, Berlin, Heidelberg, 311–327.
Rogers DF (2001): Motor control of airway goblet cells and glands. Respir Physiol 125(1): 129–144.
Schwarz Y, Muhanna N, Raveh D, Shaul C, Shahroor S, Peleg U, Attal P, Sichel JY (2017): Starplasty tracheostomy: case series and literature review. Eur Arch Otorhinolaryngol 274(5): 2261–2266.
Scurry WC Jr., McGinn JD (2007): Operative tracheotomy. Oper Tech Otolayngol Head Neck Surg 18(2): 85–89.
Sierra LK, King LG (2012): Artificial Airway Management. In: Burkitt Creedon JM, Davis H (eds.), Advanced Monitoring and Procedures for Small Animal Emergency and Critical Care. Wiley-Blackwell, Ames, Iowa, 318–339.
Solares C, Krakovitz P, Hirose K, Koltai P (2004): Starplasty: Revisiting a Pediatric Tracheostomy Technique. Otolaryngol Head Neck Surg 131(5): 717–722.
Stepnik MW, Mehl ML, Hardie EM, Kass PH, Reimer SB, Campbell BG, Mison MB, Schmiedt CW, Gregory CR, Hobson HP (2009): Outcome of permanent tracheostomy for treatment of upper airway obstruction in cats: 21 cases (1990–2007). J Am Vet Med Assoc 234(5): 638–643.
Thompson DM, Willging JP, Cotton RT (2012): Chapter 65 – Lesions of the Larynx, Trachea, and Upper Airway. In: Coran AG (ed.), Pediatric Surgery. 7th ed. Mosby, Philadelphia, 837–854.
Thurnher D (2020): Pediatric Tracheotomy. In: Klemm E, Nowak A (eds.), Tracheotomy and Airway. A Practical Guide. Springer Nature Switzerland, 57–70.
Tobias KM, Johnston SA (2018): Section 8: Trachea and Bronchi. In: Johnston SA, Tobias KM (eds.), Veterinary Surgery: Small Animal Expert Consult. 2nd ed. Saunders Elsevier, St. Louis, 1969–1982.
Vincenti S, Betting A, Durand A, Campos M, Scanziani E, Martin S (2021): Total laryngectomy in a cat with a laryngeal peripheral nerve sheath tumor. Vet Surg 50(7): 1533–1541.
Volsko TA, Parker SW, Deakins K, Walsh BK, Fedor KL, Valika T, Ginier E, Strickland SL (2021): AARC Clinical Practice Guideline: Management of Pediatric Patients With Tracheostomy in the Acute Care Setting. Respir Care 66(1): 144–155.
Watters K, O‘Neill M, Zhu H, Graham RJ, Hall M, Berry J (2016): Two-year mortality, complications, and healthcare use in children with medicaid following tracheostomy. Laryngoscope 126(11): 2611–2617.
Watters KF (2017): Tracheostomy in Infants and Children. Respir Care 62(6): 799–825.
Weissengruber GE, Forstenpointner G, Peters G, Kübber-Heiss A, Fitch WT (2002): Hyoid apparatus and pharynx in the lion (Panthera leo), jaguar (Panthera onca), tiger (Panthera tigris), cheetah (Acinonyx jubatus) and domestic cat (Felis silvestris f. catus). J Anat 201(3): 195–209.
Westhorpe RN (1987): The position of the larynx in children and its relationship to the ease of intubation. Anaesth Intens Care 15(4): 384–388.
Whitsett JA (2018): Airway Epithelial Differentiation and Mucociliary Clearance. Ann Am Thorac Soc 15(Suppl 3): 143–148.
Widdicombe J, Wine J (2015): Airway Gland Structure and Function. Physiol Rev 95: 1241–1319.
Wine JJ, Joo NS (2004): Submucosal Glands and Airway Defense. Proc Am Thorac Soc 1(1): 47–53.

Kostenfreier Download
Klicken Sie hier, wenn Sie das PDF KTP_07-2022_Zimmermann.pdf (0.37 MB) herunterladen möchten
Kostenfreier Download
Klicken Sie hier, wenn Sie das PDF KTP_07-2022_Zimmermann-Tabelle1.pdf (0.03 MB) herunterladen möchten
Kostenfreier Download
Klicken Sie hier, wenn Sie das PDF KTP_07-2022_Zimmermann-Tabelle2.pdf (0.04 MB) herunterladen möchten

{kind=link}
{kind=link}
{kind=link}