

Zum Wohle des Patienten? Über legitime und illegitime Formen der Förderung gesundheitsbezogener Interessen
Berliner und Münchener Tierärztliche Wochenschrift 133
DOI: 10.2376/0005-9366-19051
© Schlütersche Verlagsgesellschaft mbH & Co. KG. 2020
Publiziert: 05/2020
Summary
The aim of this paper is to clarify the theory of the animal patient presented in a former paper by Thurner et al. (2018) and use it as an analytical tool in veterinary ethics. By means of the case of an animal’s broken leg, which I assume can be “treated” either by splinting or by euthanasia, I demonstrate that this theory faces a structural challenge. According to the theory of Thurner et al. (2018), the performance of both treatments would make the animal a patient. This follows from the concept of promoting health-related interests as used by the authors. Therefore, in four steps, I specify the concept of promoting animals’ health-related interests with the case of the fracture. In the first step, I point out that different treatment options correspond to differing ends. In the second step, I argue that from the animal’s supposed point of view splinting the fracture is preferable to euthanasia, for this course of action promotes the animal’s best interest. In the third step, I distinguish between a legitimate and an illegitimate promotion of animals’ health-related interests. I argue that an animal qualifies as a patient only if her health-related interests are legitimately promoted. In the fourth step, I present my modified criterion for becoming a patient. In addition, I highlight two benefits of theorising the patient in veterinary ethics. First, the concept can be used to distinguish five categories of veterinary interventions. Second, the concept can stimulate changes in how humans treat animals, thereby improving animal welfare.
Zusammenfassung
Ziel dieses Aufsatzes ist es, die in einem früheren Paper von Thurner et al. (2018) dargelegte Theorie des tierlichen Patienten zu präzisieren und als analytisches Tool in der veterinärmedizinischen Ethik zu verwenden. Am Beispiel eines Tieres mit gebrochenem Bein weise ich auf ein strukturelles Problem hin, mit dem diese Theorie konfrontiert ist. Angenommen, die Fraktur könnte entweder durch das Schienen des Beins oder die Euthanasie des Tieres „behandelt“ werden, so würden beide Behandlungen das Tier nach Thurner et al. (2018) zu einem Patienten machen. Dieser Umstand ist auf das Konzept der Förderung gesundheitsbezogener Interessen zurückzuführen, dessen sich die Autoren bedienen. Ich spezifiziere daher das Konzept der Förderung gesundheitsbezogener Interessen anhand des Falls der Fraktur in vier Schritten. Im ersten Schritt zeige ich auf, dass verschiedene Behandlungsoptionen mit verschiedenen Zwecken korrespondieren. Im zweiten Schritt argumentiere ich, dass aus der mutmaßlichen Perspektive des Tieres das Schienen der Fraktur der Euthanasie vorzuziehen ist, weil diese Option das beste Interesse des Tieres fördert. Im dritten Schritt unterscheide ich eine legitime und illegitime Förderung gesundheitsbezogener Interessen. Ich argumentiere, dass ein Tier nur dann als Patient bezeichnet werden kann, wenn seine gesundheitsbezogenen Interessen legitim gefördert werden. Im vierten Schritt präsentiere ich das modifizierte Kriterium, das erfüllt sein muss, um von einem tierlichen Patienten sprechen zu können. Zudem hebe ich hervor, welche Vorteile es hat, den Patientenbegriff in der veterinärmedizinischen Ethik zu thematisieren. Erstens können mithilfe des Patientenbegriffs fünf Kategorien veterinärmedizinischen Handelns unterschieden werden. Zweitens kann der Patientenbegriff eine Änderung des Umganges mit Tieren anregen und auf diese Weise tierliches Wohlbefinden verbessern.
The theory of the animal patient: a structural challenge
In this paper, I clarify a theory of the animal patient that operates on a descriptive level. It defines the concept of the patient by referring to the ways animals are treated in veterinary practice. In this context, “treating” comprises not only the pure act of treatment by medical means but also the preceding examination of the animal by a veterinarian. Hitherto, the theory of the animal patient I am referring to has been developed in two steps. In the first step, Grimm and Huth (2017) argue that considering an animal as a patient is linked to respecting the animal’s moral status in veterinary practice. One respects an animal’s moral status by treating the animal for her own and not for others’ (e.g. the animal owner) sakes. Thus, an animal is a patient if and only if the veterinary intervention she receives aims at promoting her health-related interests for her own sake and not for others’ sakes (Grimm and Huth 2017, 225). In the second step, Thurner, Huth and Grimm (2018) demonstrated that linking the concept of the patient to respecting animals’ moral status – as Grimm and Huth (2017) have done before – is mistaken. The core of their modified theory of the animal patient is the following claim: An animal qualifies as a veterinary patient if and only if a veterinarian treats her with the end of promoting the animal’s health-related interests for her own or for others’ sakes (Thurner et al. 2018, 262). Consequently, there are patients whose moral status is respected and patients whose moral status is disrespected. For instance, an injured dog treated by a veterinarian to restore the dog’s health is a patient whose moral status is respected (Thurner et al. 2018, 264). By contrast, a dairy cow suffering from mastitis which is treated by a veterinarian to restore the cow’s capacity to produce milk is a patient whose moral status is disrespected (Thurner et al. 2018, 264).
However, the theory of Thurner et al. (2018) faces a structural challenge that refers to another dimension of the concept of the animal patient. I illustrate this challenge by means of a case, which I borrow from Rollin (2006a, 44) and adapt for the purpose of my argument. Let us suppose that some animal suffers or feels pain (used synonymously in this context) because she has a broken leg. As I address a structural challenge, it does not matter whether we take a farm animal, a companion animal, or even a wild animal. We assume that it is in the animal’s health-related interests that her suffering stops. Let us further suppose that there are two medical treatments available to end the animal’s suffering: A veterinarian can either cure the fracture by splinting the leg and prescribing the animal pain killers or she can euthanise the animal. At this point it has to be remarked that I present a conceptual argument. Therefore, I disregard legal aspects that might prohibit the performance of euthanasia in such cases. Such laws apply for instance in Austria and Germany. On the basis of Thurner, Huth and Grimm’s (2018) theory of the animal patient, not only splinting the fracture but also the performance of euthanasia would make the animal a patient. Both treatments end the animal’s suffering and thereby promote the animal’s health-related interests. This conclusion is deeply counterintuitive for the two measures are evidently not of equal value to the animal. Whereas splinting the fracture enables the animal to recover, euthanasia ends the animal’s life.
Obviously, the argument of Thurner et al. (2018) for “how to become an animal patient” needs clarification with regard to the promotion of health-related interests. I seek to accomplish this task by specifying the concept of the patient by means of distinguishing legitimate and illegitimate forms of promoting health-related interests. The aim of this paper is to develop a revised concept of the animal patient that can be used as an analytical tool in veterinary ethics. I present my argument in four steps. In the first step, I demonstrate that splinting the fracture and euthanising the animal correspond to differing ends. In the second step, I argue on the basis of the animal’s best interest that splinting the fracture is preferable to euthanasia. In the third step, I explain why splinting the fracture legitimately promotes the animal’s health-related interests while performing euthanasia does so in an illegitimate way. In the fourth step, I reformulate the criterion for becoming a patient and discuss two benefits of theorising the animal patient: First, the concept can be used to distinguish five types of veterinary interventions. Second, the concept of the animal patient has the potential to improve animal welfare.
The differing ends of veterinary medicine
In the first step, I specify the promotion of health-related interests by means of the ends of veterinary medicine. Although Thurner, Huth and Grimm’s (2018) theory of the veterinary patient modifies Grimm and Huth’s (2017) first approach, they stick to a main premise of Grimm and Huth’s initial argument. Referring to Pellegrino (1999), Grimm and Huth claim that an animal can only be considered a patient if the treatment she receives complies with the end of medicine: “[W]e can only refer to animals as patients as long as they are treated with regard to medicine’s end, which is to protect and promote health-related interests” (Grimm and Huth 2017, 225). The requirement that a veterinary intervention realises medicine’s ends by promoting an animal’s health-related interests becomes a necessary, but not sufficient criterion for the argument presented in this paper.
There is an ongoing debate in human medicine about the “ends” (Pellegrino 1999) or, more broadly speaking, “goals” (e.g. Boorse 2016, Varelius 2006) of medicine. In an effort to structure the complex discourse, Schramme (2017) introduces the distinction between a teleological and a consensual approach to determining the goals of medicine. The teleological approach understands medicine as a practice that aims at a telos, i.e. a specific end. As an advocate of this approach, Schramme (2017) cites Pellegrino (1999), who differentiates between the ends and goals of medicine. It is worth noting that Pellegrino (1999) offers a distinction closely resembling Schramme’s (2017) by differentiating between essentialist and constructionist definitions of medicine’s objectives. From Pellegrino’s (1999) point of view, ends but not goals are appropriate for depicting medicine’s objectives. The ends are embodied in medicine’s nature and hence are deduced from its essence. Pellegrino describes medicine’s end(s) as follows: “Its end is to heal, help, care and cure, to prevent illness, and cultivate health” (Pellegrino 1999, 62). As paradigmatic example of the consensual approach, Schramme (2017) quotes the list of medicine’s goals formulated by the Hastings Center (1996). The main characteristic of the consensual approach is that the goals of medicine are the product of a community’s consensus and can thereby vary with social change. In this manner, the Hastings Center identified four goals of medicine. First, “[t]he prevention of disease and injury and the promotion and maintenance of health” (Hastings Center 1996, 10). Second, “[t]he relief of pain and suffering caused by maladies” (Hastings Center 1996, 11). Third, “[t]he care and cure of those with a malady, and the care of those who cannot be cured” (Hastings Center 1996, 12). And finally, “[t]he avoidance of premature death and the pursuit of a peaceful death” (Hastings Center 1996, 13). Schramme concludes that it is in principle impossible to elaborate a precise definition of the goals of medicine for the goals depend on the concept of medicine. As medicine cannot be determined exactly, the goals of medicine cannot be determined exactly either (Schramme 2017, 123f.). However, based on the various definitions provided above, I argue that it makes sense at least to consider cure, care and the prevention of pain and disease as three ends of human medicine. This list of ends is not exhaustive, for it can be extended.
What about veterinary medicine? On account of the changed status of (companion) animals (Rollin 2011, 653ff.), who are increasingly viewed as family members (e.g. Greenebaum 2004), the ends of human medicine and companion animal medicine are getting closer to each other (Grimm et al. 2018, 1). These developments indicate that veterinary medicine shares the ends of human medicine. This poses the question: what additional ends of veterinary medicine distinguish it from human medicine? A relevant candidate is the performance of euthanasia. It is a subject of controversial discussion whether euthanasia belongs to the realm of human medicine. While some commentators endorse this view (e.g. Beauchamp and Childress 2013, 185), others strongly disagree (e.g. Pellegrino 2005, 475). By contrast, euthanasia is generally acknowledged as a legitimate “treatment” in veterinary medicine under certain conditions (Grimm et al. 2018, 3, Sandøe et al. 2016, 197, Yeates 2010, 70). According to Rollin, euthanasia is even praised as a “gift” (2011, 652) that distinguishes veterinary medicine from human medicine in many countries: “Whereas human physicians are not empowered to help horribly suffering patients end their pain by providing access to euthanasia, veterinarians are fortunately blessed to be able to end suffering by providing a peaceful and painless death” (Rollin 2011, 652). The legitimacy of performing euthanasia in veterinary practice is reflected in the “Principles of Veterinary Medical Ethics” formulated by the American Veterinary Medical Association (AVMA 2016). The second of these principles emphasises a veterinarian’s duty to “provide competent veterinary medical care” (AVMA 2016) and encompasses among other things the following stipulation: “Humane euthanasia of animals is an ethical veterinary procedure” (AVMA 2016). This specification of veterinary medical care with regard to euthanasia could indicate that euthanasia surpasses care – by relieving pain and suffering – as an end of veterinary medicine. Hence, one could consider euthanasia as the fourth end of veterinary medicine, an end that is independent of the other three ends cure, care and prevention. However, this suggestion also meets with opposition. Often, the performance of euthanasia is not perceived as an end but as “an act to end discomfort” (McMillan 2001, 1205) or, as Rollin indicates with reference to McMillan (2001), “a means to ending suffering” (Rollin 2006b, 1015).
What implications does the debate on the ends of veterinary medicine have for the case of an animal’s broken leg sketched at the beginning? Well, it clearly indicates that the promotion of the animal’s health-related interests by the performance of these two measures corresponds to differing ends, if not of veterinary medicine then at least of acting. While splinting the fracture aims at the end of cure, the performance of euthanasia corresponds to the end of ending suffering. The crucial point is that both treatment options promote the animal’s health-related interests by completely different means that have different consequences for the animal. Splinting the fracture ends the animal’s suffering by getting down to the root of the medical problem that causes the suffering and restoring the animal’s health. Euthanasia, on the other hand, ends the animal’s suffering by actively taking the animal’s life. Obviously, from the animal’s supposed point of view, the performance of these two treatment options is not of equal value. It makes a difference for the animal whether her suffering is either ended by getting down to the root of the suffering, which allows for recovery, or by ending her life. Thus, from the animal’s perspective, there is a hierarchy inherent in aiming at different ends by promoting the animal’s health-related interests. For this reason, I focus on the animal’s supposed point of view to ascertain how available medical interventions have to be weighed from the animal’s perspective.
Top Job:
Top Job:

Themenheft Tiermedizinische Ethik
Quality of life considerations and the patient’s best interest
At least in the clinic, veterinary medicine becomes increasingly patient-centred through companion animal practice (Grimm et al. 2018, Pierce and Shanan 2017b, 28, Yeates 2013, 8f.). According to Pierce and Shanan, patient-centred veterinary care requires taking the animal’s point of view into account by respecting her interests: “[T]he objective of patient-centered care […] [is] making decisions that respect patients’ wants, needs, and preferences” (Pierce and Shanan 2017b, 28). However, fulfilling this requirement is challenging because animals cannot articulate their interests and cannot take part in veterinary decision-making processes themselves (Pierce and Shanan 2017a, 58). As obtaining informed consent from an intervention’s receiving end is impossible, veterinary practice necessitates the participation of three parties in owned animals: an animal (the first party) who is taken to the veterinarian (the second party) by the owner (the third party) who becomes the veterinarian’s client by making use of the veterinarian’s services. Together, the veterinarian and the owner reach a treatment decision for the animal in virtue of the animal’s incapability to consent to medical interventions. This structure has been termed the “’therapeutic triad’” (Pierce and Shanan 2017a, 68) or “vet-patient-client triad” (Kimera and Mlangwa 2016, 2937) in veterinary practice. To prevent the animal’s interests from being overridden by the owner’s or the veterinarian’s interests, a criterion is required that integrates the animal’s supposed point of view in the decision-making process. In this respect, Pierce and Shanan refer to the animal’s quality of life which they identify as “Key to Patient-Centered Care” (Pierce and Shanan 2017b, 28). By taking the animal’s quality of life into consideration, one is adopting the animal’s perspective and is therefore in a position to determine and respect the animal’s interests.
The urgent question then is how “quality of life” should be understood. Pierce and Shanan give the following answer: “QOL [i.e.: quality of life] reflects how an animal’s physical, emotional, and social well-being is affected by disease, disability, or changes related to advanced age. Assessing QOL involves tracking of the balance between negative emotional states and positive emotional states experienced by the patient” (Pierce and Shanan 2017b, 31). Hence, the heart of the concept of quality of life involves weighing up an individual’s positive and negative states to ascertain which outweighs the other. In this calculation physical, psychological and social aspects are included (Pierce and Shanan 2017b, 32). What is striking is the fact that this definition of quality of life is explicitly tailored to sick, disabled or aging animals. Quality of life serves the assessment of how an animal experiences and handles the change of her living conditions caused by disease, disability or age. Consequently, the adoption of an animal’s point of view on the basis of this concept of quality of life is restricted to cases of sick, disabled or aging animals. Actually, this restriction is considered a common feature of the notion of quality of life: “The term ‘quality of life’ is principally used to refer to people or companion animals who are ill or recovering from illness” (Broom 2014, 34).
Correspondingly, the academic discourse on animals’ quality of life often concentrates on particular disease-related contexts. For instance, the discussion centres around end-of-life decisions (e.g. Knesl et al. 2017, Rollin 2006b, Villalobos 2011), chronic pain (e.g. Belshaw and Yeates 2018, Reid et al. 2018, Wiseman-Orr et al. 2004) or overtreatment (e.g. Grimm et al. 2018, Sandøe et al. 2016, 194f., Taylor et al. 2018). However, the adoption of an animal’s perspective in veterinary decision-making processes requires a broader understanding of quality of life. This concept of quality of life also requires balancing an animal’s positive and negative states, but it is not limited to specific disease-related contexts. Such a broad concept of quality of life is dealt with in a comparatively small amount of publications (e.g. Broom 2007 and 2014, Lavan 2013, Loftus 2013, Mullan 2015). Mullan (2015) offers a helpful starting point by equating animals’ quality of life with animal welfare. She emphasises the potential of routine quality of life assessment in veterinary practice to promote animal welfare (Mullan 2015, 207). Similarly, Broom defines an animal’s quality of life as her “welfare during a period of at least a few days” (2007, 3). Yeates confirms the importance of animal welfare as a fundamental value in veterinary medicine by appealing to veterinarians’ “duty to perform welfare-focused practice” (2013, 8). He states that the “core aims of veterinary work overlap considerably, if not entirely, with animal welfare concerns” (Yeates 2013, 1). Veterinarians’ declaration of loyalty to animal welfare is also a central component of veterinary oaths (e.g. AVMA n.d.), ethical codes (e.g. AVMA 2016, BTK 2015) and strategy papers (e.g. BVA 2016). Thus, it is veterinary medicine’s mission as a profession not solely to promote animals’ health-related interests but to promote these interests in a way that improves animals’ quality of life in terms of welfare. Therefore, I argue that the adoption of an animal’s point of view requires that the assessment of her quality of life in terms of welfare is routinely integrated in veterinary decision-making processes.
What conclusion can be drawn from these findings for the case of the animal’s broken leg? Obviously, what must be assessed is how the animal’s quality of life in terms of welfare is influenced by the performance of each treatment. This assessment is conducted in three steps. In the first step, it is assessed how each of the available interventions influences the animal’s quality of life before and after its performance. In the second step, the respective outcomes are compared. In the third step, it is ascertained on the basis of this comparison which intervention is indicated and thus has to be performed. The crucial question that remains to be answered is the following: Which criterion guides the process of prioritising the available veterinary interventions?
I suggest that the animal’s quality of life in terms of welfare should be taken into account in veterinary practice by meeting the animal’s best interest in her context. This view is supported by Grimm et al. (2018) who identify meeting an animal’s best interest as the central norm underlying the patient-centeredness of care in companion animal practice. Concurringly, Sandøe et al. (2016, 191) hold that acting in the animal’s best interests expresses a patient-centred stance as opposed to a “client-focused” (Yeates 2013, 8) or “vet-focused” (Yeates 2013, 8) stance in veterinary practice. Sandøe et al. (2016, 191) stress that the principle of meeting the patient’s best interests has been derived from human medicine. In this context, it guides decision-making processes for human patients who cannot consent to medical interventions like children, severely cognitively disabled or comatose humans. As one cannot obtain informed consent from animals either, the necessity of meeting the patient’s best interests can be adopted as a model for decision-making processes in veterinary medicine (Sandøe et al. 2016, 191). But how can the abstract principle of acting in the patient’s best interest be translated into instructions for veterinary practice?
I deem it necessary to reject a consequentialist understanding of best interest like the one Beauchamp and Childress (2013) add to human medical ethics. According to their view, “best interest” is the one treatment option with “the highest probable net benefit” (Beauchamp and Childress 2013, 228) for the patient. Also, reaching treatment decisions in veterinary practice requires prioritising all available treatment options with regard to the animal’s interests. However, a consequentialist notion of best interest would entail that among all available treatment options only one option is in the animal’s best interest. As the effects of some treatment options for an animal’s welfare might differ insignificantly, such a narrow account of best interest is counterintuitive. By contrast, I advocate an ex negative definition of best interest that I adopt from Ashall et al. (2018): “Crucially, doctors […] are obliged to act in the best interests of their patient only and third party consent cannot be used against the patient’s interests” (Ashall et al. 2018, 251). A performance of any intervention is in the patient’s best interest when it does not violate the patient’s interests. Consequently, it is possible that more than one treatment option is in the animal patient’s best interest. Hence, the term “best interest” refers to the animal’s supposed interests as paternalistically identified by the veterinarian.
Based on this approach, the case of an animal’s broken leg can be analysed as follows. Although not only splinting the fracture but also performing euthanasia promotes the animal’s health-related interests, splinting the fracture is the indicated treatment option from the animal’s supposed point of view. Although euthanasia also qualifies as a suitable means to end the animal’s suffering, it would kill the animal. As splinting the leg is an equally effective means to end the suffering but makes recovery possible, this course of action is in the animal’s best interest. In the next section, I frame these findings with the concepts of the legitimate and illegitimate promotion of health-related interests and examine their implications for conceptualising the animal patient.
Legitimate vs. illegitimate promotion of health-related interests
At the beginning, I presented the case of the fracture, which is a structural challenge to Thurner, Huth, and Grimm’s (2018) theory of the animal patient. This theory confers the status of patient to an animal if and only if the animal’s health-related interests are promoted by a veterinary intervention. In general terms, the structural challenge to this theory can be expressed as follows: An animal qualifies as a patient even though the animal’s health-related interests are promoted by a veterinary intervention in a way that does not meet her best interest.
Considering my analysis of the case of the fracture, I conclude that the pure act of promoting health-related interests does not make an animal a patient. From the animal’s point of view, the concept of promoting health-related interests has to be specified by distinguishing two different forms. The first form is the legitimate promotion of health-related interests. The promotion of health-related interests is legitimate if it is justified from a moral point of view. Health-related interests are legitimately promoted by a veterinarian if the performed veterinary intervention promotes an animal’s health-related interests by meeting the animal’s best interest. Hence, acting in an animal’s best interest is a specific form of promoting the animal’s health-related interests. I argue that an animal solely qualifies as a patient if her health-related interests are legitimately promoted by a veterinary intervention. This thesis can be supported with Grimm et al. (2018). They identify acting in an animal’s best interest as the central norm underlying patient-centred veterinary practice. Thus, the authors declare that acting in an animal’s best interest is a morally justificatory reason for veterinary interventions. If the performance of a veterinary intervention meets an animal’s best interest, the intervention is justified in a moral sense. As performing a veterinary intervention that legitimately promotes an animal’s health-related interests is morally justified for acting in the animal’s best interest, the animal is a patient. With regard to the case of the fracture, this applies to splinting the leg. This treatment option promotes the animal’s health-related interests legitimately as it is in the animal’s best interest. Therefore, splinting the fracture makes the animal a patient.
The second form of promoting health-related interests is the illegitimate promotion of health-related interests. The promotion of health-related interests is illegitimate if it is not justified from a moral point of view. Health-related interests are illegitimately promoted by a veterinarian if the performed veterinary intervention promotes an animal’s health-related interests against the animal’s best interest. The illegitimate promotion of an animal’s health-related interests clearly violates the central norm of patient-centred veterinary practice. Grimm et al. (2018) remark that interventions acting against animals’ best interests are performed for secondary reasons like making money or training young colleagues. Thus, they describe secondary reasons as explanatory reasons for veterinary interventions. Secondary reasons explain why veterinary interventions are performed but they do not justify them in a moral sense. As performing a veterinary intervention that illegitimately promotes an animal’s health-related interests lacks a moral justification for it acts against the animal’s best interest, the animal cannot be referred to as a patient. With regard to the case of the fracture, this applies to euthanising the animal. Although this “treatment” option promotes the animal’s health-related interests, it does so illegitimately for it acts against the animal’s best interest. Therefore, the animal cannot be considered a patient when euthanised. In the last section, I consider the potential of conceptualising the animal patient in veterinary ethics.
Implications of theorising the animal patient
Based on the argument presented in this paper, the criterion for becoming an animal patient has to be clarified as follows: An animal is a patient if and only if the end of a veterinary intervention is to legitimately promote the animal’s health-related interests by meeting her best interest, either for her own or for others’ sakes. If an animal’s health-related interests are illegitimately promoted by a veterinary intervention because it acts against the animal’s best interest, the animal cannot be considered a patient.
At this point it can be objected that elaborating a theory of the animal patient is one thing, but the pressing question is what is gained by adequately conceptualising the animal patient. What is the good of distinguishing patients and non-patients in veterinary practice at all? I argue that the concept of the animal patient enriches the discourse in veterinary ethics in at least two respects. First, the concept functions as a useful tool to classify veterinary interventions. Second, the concept of the animal patient possesses the normative potential to improve animal welfare by stimulating changes concerning the treatment of animals. In the following, I spell these points out in detail.
Categorising veterinary interventions
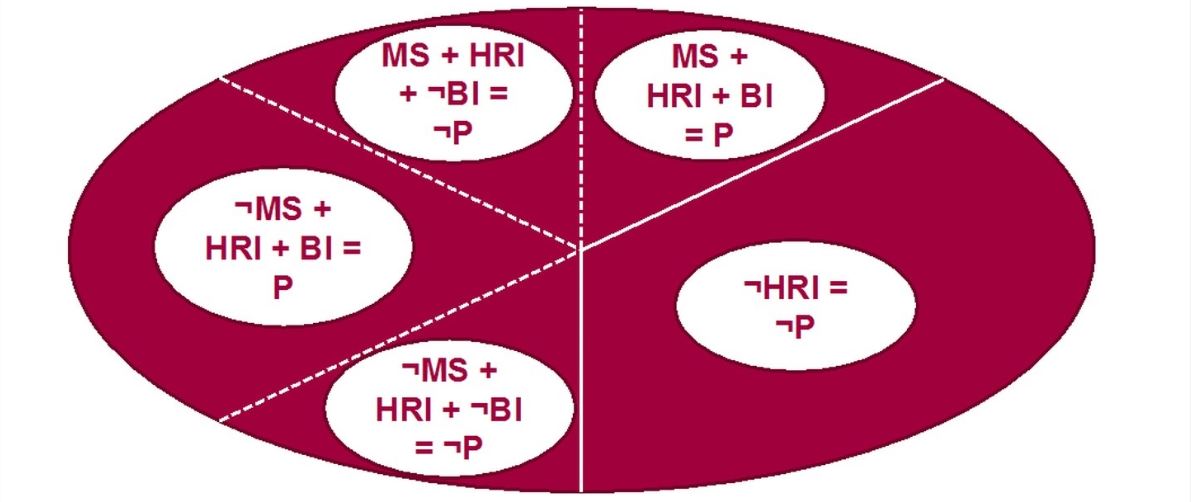
First of all, the concept of the animal patient can be used as a tool to distinguish different categories of veterinary interventions. By means of the concept of the animal patient, I outline five different types of veterinary interventions that are performed by veterinarians referring to Figure 1. In a first step, veterinary interventions have to be divided into interventions that either promote animals’ health-related interests (HRI, Fig. 1) or do not promote animals’ health-related interests (¬HRI, Fig. 1). I have stated that the promotion of an animal’s health-related interests is a necessary but not sufficient criterion for being a patient. Therefore, the performance of veterinary interventions that do not promote animals’ health-related interests (¬HRI) makes animals non-patients (¬P). An example for this category of veterinary intervention is the case of male piglets who are castrated by a veterinarian that is described by Thurner et al. (2018, 261 and 264). As the procedure is not performed to promote the piglets’ health-related interests but to meet consumers’ aesthetic interests, who dislike boar tainted meat, the piglets cannot be declared patients.
However, promoting animals’ health-related interests is not a sufficient criterion for being a patient. For this reason, the category of veterinary interventions that promote animals’ health-related interests needs to be divided into four subcategories:
(1) There are veterinary interventions that respect an animal’s moral status (MS) for being performed for the animal’s sake and promote the animal’s health-related interests (HRI) by meeting her best interest (BI). By the performance of such interventions, an animal’s health-related interests are legitimately promoted and hence the animal qualifies as a patient (P). This kind of veterinary intervention is primarily performed in companion animal clinics. An example would be an injured cat who receives treatment by a veterinarian. The cat is treated for her own sake and receives a treatment that promotes her health-related interests by meeting her best interest. Thus, the cat is a patient.
(2) There are veterinary interventions that respect an animal’s moral status (MS) for being performed for the animal’s sake but promote the animal’s health-related interests (HRI) in a way that acts against the animal’s best interest (¬BI). By the performance of such interventions an animal’s health-related interests are illegitimately promoted and hence the animal does not qualify as a patient (¬P). This kind of veterinary intervention is also mainly performed in companion animal clinics. This is, for instance, the case when an intervention is performed on an animal upon the owner’s request although the veterinarian considers it less effective with regard to the animal’s best interest than another treatment option. An example for this category of veterinary intervention is the case of male piglets who are castrated by a veterinarian that is described by Thurner et al. (2018, 261 and 264). What is at stake here is not the effectiveness of alternative treatment methods, but the veterinarian being forced to perform an intervention that – according to her – does not meet the animal’s best interest. Although the cat is treated for her own sake, her health-related interests are promoted against her best interest. For this reason, she cannot be referred to as a patient.
(3) There are veterinary interventions that disrespect an animal’s moral status (¬MS) for being performed for others’ sakes but promote the animal’s health-related interests (HRI) by meeting the animal’s best interest (BI). Although the animal’s moral status is disrespected, her health-related interests are legitimately promoted by the performance of such interventions. Therefore, the animal is a patient (P). This category of veterinary intervention is primarily relevant in farm animal practice. A typical example is the case of a dairy cow whose mastitis is treated by a veterinarian that is described by Grimm and Huth (2017, 225) as well as Thurner et al. (2018). The mastitis is not cured for the cow’s but for the farmer’s sake who has an economic interest in restoring the cow’s capacity to produce milk that can be sold. Nevertheless, curing the mastitis promotes the cow’s health-related interests in a way that meets her best interest, which makes her a patient.
(4) There are veterinary interventions that disrespect an animal’s moral status (¬MS) for being performed for others’ sakes and promote the animal’s health-related interests (HRI) in a way that acts against the animal’s best interest (¬BI). As the animal’s health-related interests are illegitimately promoted, the animal cannot be referred to as a patient (¬P). This type of intervention is often performed in farm animal practice but also occurs in companion animal practice by performing certain forms of convenience euthanasia. The latter denotes the killing of healthy animals that lacks medical indication and is performed for secondary reasons (Rollin 2011, 652). An example for this category of veterinary intervention is the case of the broken leg discussed in this paper that is inspired by Rollin (2006a, 44). Let us assume that a sow’s fracture is not splinted, but the animal is euthanised solely for economic reasons. In this case, the euthanasia is performed for the farmer’s sake and clearly promotes the sow’s health-related interests illegitimately, i.e. against her best interest. Therefore, the sow cannot be considered a patient.
The classification of veterinary interventions helps us understand why adopting an animal rights-based approach to veterinary practice is highly problematic. As such an approach calls for respecting animals’ moral status, it approves only one type of intervention veterinarians regularly perform. From an animal rights perspective, solely performing veterinary interventions that respect animals’ moral status and promote their health-related interests by meeting their best interests is morally permissible. However, veterinary practice is not reducible to this specific type of intervention,
which might be considered the veterinary ideal of treating animals. Rather, veterinary practice consists in the performance of all five types of interventions, which lays the foundation of various tensions and problems.
As the concept of the patient has demonstrated,
veterinarians have – among other things – the professional responsibility to legitimately promote animals’ health-related interests by meeting animals’ best interests. But not all interventions that veterinarians are required to perform in practice are directed at a patient. Some interventions do not promote animals’ health-related interests at all. Others promote animals’ health-related interests but do it in a way that acts against animals’ best interests. Furthermore, veterinarians are often required to perform interventions that disrespect animals’ moral status by being performed for others’ sakes. The impossibility of always fulfilling the professional duty to meet animals’ best interests in veterinary encounters can be stressful for veterinarians. This phenomenon is closely related to veterinarians’ experience of moral stress (e.g. Kipperman et al. 2018, Moses et al. 2018, Rollin 2011).
Improving animal welfare
Further, the concept of the animal patient possesses normative potential, as it can be used to point out and reflect moral problems that concern the treatment of animals. Once again, I want to illustrate this point with the case of the sow’s fracture that is inspired by Rollin (2006a, 44).As the veterinarian acts against the sow’s best interest by euthanising her, the sow does not qualify as a patient. However, it could be objected that the sow should be considered a patient. Given the husbandry conditions of industrial farming, performing euthanasia might be in the sow’s best interest after all. This is a valid yet somewhat counterintuitive argument. Still, from the sow’s point of view splinting the fracture is preferable to euthanasia, for the former restores her health whereas the latter ends her life. Rather, what the counterargument indicates is that the conditions of keeping the sow have to be questioned. Nevertheless, similar objections can be put forward with regard to numerous other cases, particularly in farm animal practice.
It is of crucial importance to note that veterinarians act as agents of common social practices that concern the treatment of animals. As such, they cannot and may under no circumstances be made responsible for morally problematic ways of treating animals that follow from these practices. Notwithstanding, veterinarians might still experience it as stressful that an animal they are treating medically is, for instance, considered a resource for human use by society. In this respect, the concept of the animal patient provides a suitable means to articulate and reflect on the general conditions that prevent veterinarians from acting in animals’ best interests. Take the case of the sow’s fracture. In this context, the concept of the patient can be used to question common husbandry conditions. So, the un-/willingness to refer to specific animals as patients may stimulate public discussions on how humans should treat animals. Such debates may result in better treatment of animals, especially if they influence legislation. Therefore, the concept of the animal patient has the normative potential to change the ways in which humans treat animals and thereby improve animal welfare.
Conclusion
This paper has two objectives. First, it aims at developing a convincing theory of the animal patient based on the conceptualisation of Thurner et al. (2018). In this paper, I clarify the criterion for becoming a patient as follows: An animal qualifies as a patient if and only if she receives a veterinary intervention that aims at the legitimate promotion of her health-related interests by meeting her best interest. My theory makes more specific the concept of promoting health-related interests that is used by Thurner et al. (2018). With regard to an animal’s perspective, I distinguished between a legitimate and an illegitimate promotion of her health-related interests by veterinary interventions. I defined legitimately promoting the animal’s health-related interests as acting in the animal’s best interest. This form of promoting the animal’s health-related interests makes the animal a patient. By contrast, I defined illegitimately promoting the animal’s health-related interests as acting against the animal’s best interest. In this case, the animal cannot be considered a patient.
The second objective of my paper is to highlight the merits of theorising the animal patient. I pointed out that there are two ways in which the concept of the animal patient enriches the discourse in veterinary ethics.
First of all, the concept of the patient can be used to differentiate between five types of veterinary interventions: (1) Veterinary interventions that do not promote the animal’s health-related interests and hence do not make the animal a patient. (2) Veterinary interventions that promote an animal’s health-related interests, respect the animal’s moral status by being performed for the animal’s sake, and further meet the animal’s best interest. This type of intervention promotes the animal’s health-related interests legitimately and hence makes her a patient. (3) Veterinary interventions that promote an animal’s health-related interests, respect the animal’s moral status by being performed for the animal’s sake, but, nevertheless, act against the animal’s best interest. This type of intervention promotes the animal’s health-related interests illegitimately and hence does not make the animal a patient. (4) Veterinary interventions that promote the animal’s health-related interests, disrespect the animal’s moral status by being performed for others’ sakes, but still meet the animal’s best interest. This type of intervention promotes the animal’s health-related interests legitimately and hence makes the animal a patient. (5) Veterinary interventions that promote an animal’s health-related interests, disrespect the animal’s moral status by being performed for others’ sakes, and act against the animal’s best interest. This type of intervention promotes the animal’s health-related interests illegitimately and hence does not make the animal a patient. Veterinary practice is not reducible to any specific type, but rather requires the performance of all five types of interventions. It might be stressful for veterinarians that not every intervention they perform promotes animals’ health-related interests legitimately by meeting the animals’ best interests.
The second benefit of theorising the animal patient is the concept’s potential to improve animal welfare. The (un-)willingness to refer to animals as patients in certain cases can stimulate public discussions on the morally appropriate ways of treating them. As these debates might result in better treatment of animals, the concept of the animal patient is capable of improving animal welfare.
Acknowledgements
I would like to thank heartily Herwig Grimm, my mentor, for supporting me in developing my argument and for his thoughtful comments on the manuscript. Also, I want to thank Andreas Aigner and Johanna Karg. Further, I am grateful to the two anonymous reviewers whose appreciative feedback helped me to improve my paper.
Conflict of interest
The author declares that she has no conflicts of interest.
Ethical approval
The author declares that she has met common international ethical guidelines concerning good scientific practice in the course of writing the above work.
Funding
No funding.
Author’s note
An earlier version of this paper was presented on January 25th, 2019 at the FU Berlin at the first conference of the Netzwerk Tiermedizinische Ethik (research network veterinary ethics).
Address for correspondence
Elena Thurner, BA
Messerli Research Institute
Unit of Ethics and Human-Animal Studies
University of Veterinary Medicine, Medical University of Vienna and University of Vienna
Veterinärplatz 1
1210 Vienna
Austria
elena.thurner@vetmeduni.ac.at
References
Ashall V, Millar KM, Hobson-West P (2018): Informed Consent in Veterinary Medicine: Ethical Implications for the Profession and the Animal ‘Patient’. Food ethics 1: 247–258.
AVMA (2016): Principles of Veterinary Medical Ethics of the AVMA. https://www.avma.org/KB/Policies/Pages/Principles-of-Veterinary-Medical… (accessed December 11, 2018).
AVMA (n.d.): Veterinarian’s Oath. https://www.avma.org/KB/Policies/Pages/veterinarians-oath.aspx (accessed November 25, 2019).
Beauchamp TL, Childress JF (2013): Principles of Biomedical Ethics. 7th ed., Oxford University Press, New York and Oxford.
Belshaw Z, Yeates J (2018): Assessment of quality of life and chronic pain in dogs. Vet J 239: 59–64.
Boorse C (2016): Goals of Medicine. In: Giroux É (ed.), Naturalism in the Philosophy of Health. Issues and Implications. Springer, Switzerland, 145–177.
Broom DM (2007): Quality of life means welfare: how is it related to other concepts and assessed? Anim Welf 16 (suppl): 45–53.
Broom DM (2014): Sentience and Animal Welfare. CABI, Wallingford and Boston.
BTK (2015): Ethik-Kodex der Tierärztinnen und Tierärzte Deutschlands. https://www.bundestieraerztekammer.de/btk/ethik/ (accessed November 25, 2019).
BVA (2016): Vets speaking up for animal welfare. BVA (British Veterinary Association) animal welfare strategy. https://www.bva.co.uk/media/3124/bva-animal-welfare-strategy-final-vers… (accessed December 19, 2019).
Greenebaum J (2004): It’s a Dog’s Life: Elevating Status from Pet to “Fur Baby” at Yappy Hour. Soc Anim 12: 117–135.
Grimm H, Bergadano A, Musk GC, Otto K, Taylor PM, Duncan JC (2018): Drawing the line in clinical treatment of companion animals: recommendations from an ethics working party. Vet Rec 182: 664, DOI 10.1136/vr.104559.
Grimm H, Huth M (2017): One Health: Many Patients? A short theory on what makes an animal a patient. In: Jensen-Jarolim E (ed.), Comparative Medicine. Disorders linking humans with their animals. Springer, Cham, 219–230.
Hastings Center (1996): The Goals of Medicine. Setting new priorities. Hastings Cent Rep 26: 1–27.
Kimera SI, Mlangwa JED (2016): Veterinary Ethics. In: ten Have H (ed.), Encyclopedia of Global Bioethics. Springer Reference, Switzerland, 2937–2947.
Kipperman B, Morris P, Rollin B (2018): Ethical dilemmas encountered by small animal veterinarians: characterisation, responses, consequences and beliefs regarding euthanasia. Vet Rec 182: 548, DOI 10.1136/vr.104619.
Knesl O, Hart BL, Fine AH, Cooper L, Patterson-Kane E, Houlihan KE, Anthony R (2017): Veterinarians and Humane Endings: When is it the right time to euthanize a companion animal? Front Vet Sci 4: 45, DOI 10.3389/fvets.2017.00045.
Lavan RP (2013): Development and validation of a survey for quality of life assessment by owners of healthy dogs. Vet J 197: 578–582.
Loftus L (2013): Equine quality of life assessment: a review of protocol and practice. Veterinary Nursing Journal 28: 392–395.
McMillan FD (2001): Rethinking euthanasia: death as an unintentional outcome. J Am Vet Med Assoc 219: 1204–1206.
Moses L, Malowney MJ, Wesley Boyd J (2018): Ethical conflict and moral distress in veterinary practice: A survey of North American veterinarians. J Vet Intern Med 32: 2115–2122.
Mullan S (2015): Assessment of quality of life in veterinary practice: developing tools for companion animal carers and veterinarians. Vet Med (Auckl) 6: 203–210.
Pellegrino ED (2005): Some things ought never be done: moral absolutes in clinical ethics. Theor Med Bioeth 26: 469–486.
Pellegrino ED (1999): The Goals and Ends of Medicine: How are they to be defined? In: Hanson MJ, Callahan D (eds.), The Goals of Medicine. The Forgotten Issue in Health Care Reform. Georgetown University Press, Washington, 55–68.
Pierce J, Shanan A (2017a): Ethical Decision Making in Animal Hospice and Palliative Care. In: Shanan A, Pierce J, Shearer T (eds.), Hospice and Palliative Care for Companion Animals: Principles and Practice. Wiley Blackwell, Hoboken, 57–71.
Pierce J, Shanan A (2017b): Quality of Life in the Animal Hospice and Palliative Care Patient. In: Shanan A, Pierce J, Shearer T (eds.), Hospice and Palliative Care for Companion Animals: Principles and Practice. Wiley Blackwell, Hoboken, 27–40.
Reid J, Nolan AM, Scott EM (2018): Measuring pain in dogs and cats using structured behavioural observation. Vet J 236: 72–79.
Rollin BE (2006a): An Introduction to Veterinary Medical Ethics. Theory and Cases. 2nd ed., Blackwell Publishing, Ames.
Rollin BE (2006b): Euthanasia and quality of life. J Am Vet Med Assoc 228: 1014–1016.
Rollin BE (2011): Euthanasia, moral stress, and chronic illness in veterinary medicine. Vet Clin North Am Small Anim Pract 41: 651–659.
Sandøe P, Corr S, Palmer C (2016): Companion Animal Ethics. Wiley, Chichester.
Schramme T (2017): Goals of Medicine. In: Schramme T, Edwards S (eds.), Handbook of the Philosophy of Medicine. Springer, Dordrecht, 121–128.
Taylor P, Monroe T, Murphy K, Chennells D (2018): We need to question over treatment. Vet Rec 183: 27.
Thurner E, Huth M, Grimm H (2018): Being a veterinary patient and moral status: a disentanglement of two normative dimensions. In: Springer S, Grimm H (eds.), Professionals in food chains. Wageningen Academic Publishers, Wageningen, 260–265.
Varelius J (2006): Voluntary euthanasia, physician-assisted suicide, and the goals of medicine. J Med Philos 31: 121–137.
Villalobos AE (2011): Quality-of-life assessment techniques for veterinarians. Vet Clin North Am Small Anim Pract 41: 519–529.
Wiseman-Orr ML, Nolan AM, Reid J, Scott EM (2004): Development of a questionnaire to measure the effects of chronic pain on health-related quality of life in dogs. Am J Vet Res 65: 1077–1084.
Yeates J (2010): Ethical aspects of euthanasia of owned animals. In Practice 32: 70–73.
Yeates J (2013): Animal Welfare in Veterinary Practice. Wiley-Blackwell, Oxford.


Kostenfreier Download
Klicken Sie hier, wenn Sie das PDF BMTW-10.23760005-9366-19051-Thurner.pdf (0.16 MB) herunterladen möchten




{kind=link}